All published articles of this journal are available on ScienceDirect.

Low Body Mass Index and Trends of Tuberculosis Infection: A Cohort Study of Orphan Children in Azad Jammu and Kashmir Pakistan
Authors Info & Affiliations
Abstract
Background:
The tuberculosis is one the most life-threatening poverty associate diseases affecting one-third of the world population. The objective of the present study was to evaluate the trends of tuberculosis infection, and general health conditions of orphan children in Azad Jammu and Kashmir (AJK), Pakistan.
Methods:
Total 1708 children have enrolled in this a longitudinal study and were screened for tuberculosis through sputum smear and PCR tests. Body Mass Index (BMI), exposure to tuberculosis risk factors was also analyzed for all participants.
Results:
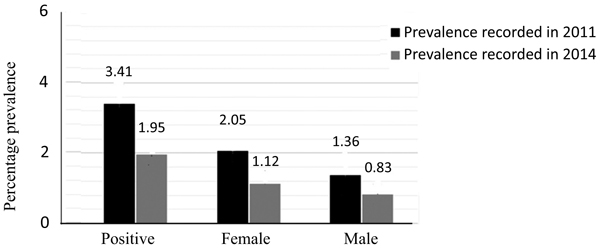
In 2011, the prevalence of tuberculosis was 3.41%, 1.36%, which was among male and 2.05% among female children. In 2015, we found 1.95% positive tuberculosis cases including 1.12% females and 0.83% males. A significant overall decline in tuberculosis infection was found in four years, p < 0.01. The mean BMI value for male and female children was 21.70 (SD±0.68) and 17.53 (SD±0.72), respectively.
Conclusion:
In conclusion, malnutrition, unhygienic and crowded living conditions are strong factors contributing to TB infection and serious threat to the orphan children, especially for the females.
1. INTRODUCTION
Tuberculosis (TB) caused by Mycobacterium tuberculosis is a pronounced menace to human health affecting about one-third of the population worldwide [1, 2]. It causes 1.5 million deaths and 9 million new cases annually [3, 4]. However, only a small proportion shows symptoms of disease [5, 6]. Since M. tuberculosis is spread by aerosol droplets, the lungs are most commonly affected by the disease [7]. It is well known that environmental exposures, such as silica dust or cigarette smoke, can increase the risk of developing TB [8-11]. TB is considered poverty and lifestyle associated disease [12, 13]. According to the estimates, the risk of TB infection is 40% higher in poor developing countries as compared to the developed countries and it contributes as the second leading cause of death among infectious diseases in the poor countries [14].
With an annual case incidence of 500,000 cases of infection, Pakistan falls 5th among the 22 countries with the highest TB cases [15]. Poor living standards, lack of basic health facilities may cause additional risk of tuberculosis by attracting the other risk factors like malnutrition, indoor living, air pollution etc. Orphan children represent a highly deprived and neglected group of the population worldwide [13]. They constitute a high-risk group for tuberculosis infection and malnutrition owing to their poor socio-economic status. Although there are several reports about the epidemiology of TB among children [16-18], little data is available about orphan children from the world generally and from Pakistan particularly. Such special groups of the population have more chances of TB infection due to living in crowded, less ventilated places, having limited safe cooking and health facilities [19, 20].
The main objective of the study was to assess the association of tuberculosis with the health conditions of poor and neglected group of children in the remote areas of Azad Jammu and Kashmir (AJK), Pakistan. In the present study, we screened orphan children living in Azad Jammu and Kashmir area of Pakistan. The study area consists of 13,297 square kilometers with a population of about 4.6 million people divided into 7 administrative districts namely, Muzaffarabad, Bagh, Kotli, Poonch, Sudhnutti, Mirpur, and Bhimber Fig. (1). This long-term analytical study was carried over 4 years. The first phase was conducted in 2011 and the second phase in 2015.

2. MATERIALS AND METHODS
2.1. Study Design
It was a cross-sectional, analytical study. A total of 1708 children between 5 to 17 years of age were included in the study from seven districts. The first phase was the initial stage for a screening of children for tuberculosis and BMI. The risk factors for tuberculosis were also assessed. The second phase started after five years to evaluate the impact of local and international health institutions. Unrelated means the children studied in the first phase were not included in the second phase.
2.2. Ethical Approval
The study protocol was approved by the Institutional Ethical Committee and Board of Advanced Studies and Research at the University of Azad Jammu and Kashmir Pakistan as notified by the university letter No. F-BASR/ (14th M)/20-73/7060-64/2011.
2.3. Inclusion and Exclusion Criteria
Male and female children living in the orphan houses or with related families, who voluntarily offered for sampling and screening were included in the present study.
2.4. Signing the Consent Form
The aims and objectives of the study were explained to the legal guardian of each child and a consent form was signed.
2.5. Sampling and Analysis by Smear Test and PCR
The blood samples were collected by venipuncture using a 5ml sterile syringe and stored in an EDTA (Ethylenediamine Tetra Acetic Acid) coated tubes at -20 ºC. Early morning sputum samples were collected and slides were prepared, stained and counterstained with Ziehl-Neelsen’s 1 percent Carbol-fuchsin solution and methylene blue respectively. The stained smear was observed under a binocular microscope with a regular objective of 40X and oil immersion objective of 100X. Those smears in which Acid-Fast Bacilli (AFB) appeared as red rods in clusters clearly visible against blue background were considered as positive. The samples were also subjected to Polymerase Chain Reaction (PCR) for confirmation of active TB. Bacterial DNA was extracted from the plasma of positive cases by using commercially available DNA extraction kits (DNAzol ®BD. Cat. No. DN129, Molecular Research Centre USA). A nested PCR was used to amplify 778 bp fragment in the first round and 151 bp fragment in the second round. The primers with nucleotide sequences 5´ gtgcggatggtcgcagag 3´ and 5´ ctcgtccagcgccgcttcg 3´ were used as forwarding primers and that with nucleotide sequences 5´cctgcgagcgtaggcgtcgg 3´ and 5´ ctcgatgccctcacggttca 3´ as reverse primers for the first and second rounds of PCR, respectively. A PCR mixture of 20 μL was prepared for the first and second round of PCR by mixing 1 mM dNTPs, 2 mM MgCl2, 1 μL each of 40 picomoles of each of the forward and reverse primers, 1x Taq polymerase buffer, 2.5 U of Taq polymerase and 20 to 40 ng of template DNA. The thermocycler was adjusted at 94ºC (denaturation) for four min, trailed by 35 cycles, each of 30 seconds at 94ºC (denaturation), 40 seconds at 45ºC (annealing) and 30 seconds at 72ºC (extension) with the final extension at 72ºC for 5 min. Samples were visualized in UV transilluminator after the electrophoresis with 2 percent agarose gel prepared in 1X TBE buffer having 10 mg/ mL concentration of ethidium bromide and subjected to electrophoresis at 120V for 40 min.
2.6. Calculation of Body Mass Index (BMI)
Weight and height of participants were measured using a stadiometer, and weighing machine, without shoes and up to maximum accuracy. The criteria of World Health Organization (WHO) for the BMI [weight / height2; (kg/m2] calculations was used (WHO, 2000). The participants with <18.50 value of BMI were considered as underweight, with 18.50 to 24.99 were considered as healthy weight, with 25.00 - 29.99 were considered as overweight and those with ≥ 30 values were considered as obese.
2.7. Analysis of Risk Factors and Hematological Parameters
Different hematological parameters were analyzed among the positive samples. Recent kit based procedures were applied for the analysis of each parameter. The risk factors associated with TB infection including, contact with infected people, consumption of raw milk, use of fossil fuel, poor ventilation, interaction with bovine and overcrowding, were also determined for all the subjects included in this investigation.
2.8. Statistical Analysis
The percentage of TB-positive samples was calculated and tabulated for all 7 districts. The variability of disease incidence among the male and female subjects was also determined. The t-test was applied for the evaluation, whether the two independent populations have the same mean or not. The p-values were calculated to indicate the chances of occurrence of prevalence. P-values less than 0.05 were considered as significant.
3. RESULTS
3.1. Descriptive Results
During the first phase of the study (in 2011), out of 733 samples, 25 samples were found positive for sputum smear test and PCR indicating 3.41% tuberculosis infection (Table 1 and Fig. 2). Four years later, in the second phase (in 2015) to analyze the effects of efforts by related government and non-government institutions, the prevalence of infection was determined among the unrelated children (Table 1). Out of 975 subjects, 19 were found positive indicating 1.95% prevalence. During the first phase, the male and female positive subjects were 1.36% and 2.05% respectively. After 4 years of the first phase, we found an active infection among 0.83% male and 1.12% female children. With the exception of Sudnutti, the decreasing trend of infection was found in tuberculosis infection in 2015 than in 2011 Table (1).
3.2. District Wise and Gender Wise Prevalence
The prevalence of tuberculosis was carried out in seven districts of Azad Jammu and Kashmir, Pakistan including Muzaffarabad and Neelum, Poonch, Bagh, Mirpur, Sudhnutti, Bhimber, and Kotli (Fig. 1). District wise and gender wise prevalence of tuberculosis are shown in Table 1.
| Districts | Total Subjects/ | Frequency and Percentage of Subjects Confirmed for Active TB by Culture and PCR Test | ||
|---|---|---|---|---|
| (Year) | ||||
| Male N (%) | Female N (%) | Total N (%) | ||
| Muzaffarabad and Neelum | 60/ (2011) | 0 | 2 (3.33%) | 2 (3.33%) |
| 70/ (2015) | 0 | 2 (2.85%) | 2 (2.85%) | |
| Poonch | 80 (2011) | 1 (1.25%) | 2 (2.50%) | 3 (3.75%) |
| 90 (2015) | 1 (1.11%) | 1 (1.11%) | 2 (2.22%) | |
| Bagh | 150 (2011) | 3 (2.00%) | 1 (0.60%) | 4 (2.60%) |
| 400 (2015) | 3 (0.70%) | 3 (0.75%) | 6 (1.50%) | |
| Mirpur | 75 (2011) | 0 | 2 (2.66%) | 2 (2.66%) |
| 85 (2015) | 0 | 1 (1.11%) | 1 (1.11%) | |
| Sudhnutti | 60 (2011) | 0 | 1 (1.66%) | 1 (1.66%) |
| 55 (2015) | 1 (1.81%) | 0 | 1 (1.81%) | |
| Bhimber | 250 (2011) | 5 (2.00%) | 6 (2.40%) | 11 (4.40%) |
| 200 (2015) | 2 (1.00%) | 2 (1.00%) | 4 (2.00%) | |
| Kotli | 58 (2011) | 1 (1.72%) | 1 (1.72%) | 2 (3.44%) |
| 75 (2015) | 1 (1.33%) | 2 (2.66%) | 3 (3.99%) | |
| Total Samples/ average percentage | 733 (2011) | 10 (1.36%) | 15 (2.05%) | 25 (3.41%) |
| 975 (2015) | 8 (0.83%) | 11 (1.12%) | 19 (1.95%) | |
3.3. Body Mass Index
The BMI of all participants indicated a nutritional deficiency. The mean BMI value for male children was 21.70 (SD±0.68) and that for female children was 17.53 (SD±0.72). Overall 53% of participants were underweight, 31% were in the healthy range and remaining were overweight. The results indicate that more females were suffering from nutritional deficiency as compared to male children.
3.4. Haematological Parameters
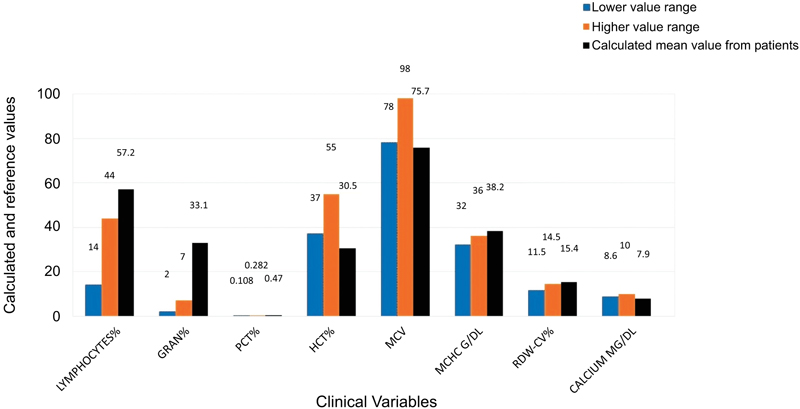
Hematological profiles of all the positive subjects revealed that some variables were elevated and some others were lower than their normal values. Lymphocytes (Lymph), Granulocytes (Gran), the relative volume of Platelet (PCT), Mean Corpuscular Hemoglobin Concentration (MCHC) and Red Cell Distribution Width (RDW-CV) were found to be significantly elevated among all the positive TB cases. While the Mean Corpuscular Volume (MCV) and Hematocrit (HCT) were found to be substantially lower among the TB positive subjects (Table 2 and Fig. 3).
| Blood Parameter | Lower Reference Range | Higher Reference Range | Calculated Mean Value |
|---|---|---|---|
| Lymphocytes % | 14 | 44 | 57.2 |
| Granulocytes % | 2 | 7 | 33.1 |
| Procalcitonin % | 0.108 | 0.282 | 0.47 |
| Hematocrit % | 37 | 55 | 30.5 |
| Mean Corpuscular Volume | 78 | 98 | 75.7 |
| Mean Corpuscular Hemoglobin Concentration (MCHC-g/dl) | 32 | 36 | 38.2 |
| Red Cell Distribution Width (RDW) | 11.5 | 14.5 | 15.4 |
| Calcium (mg/dL) | 8.6 | 10 | 7.9 |
3.5. Risk Factors
In 2011, investigation of each individual indicated that 4.4% orphans were exposed to proximity or close contact with TB patients. Raw milk consumption was common among 67% of subjects, 73% were extensively using fossil fuel, 63.3% respondents were exposed to poor ventilation and 30.5% were vulnerable to bovine contact. In 2015, the proximity to infected persons was 4%, raw milk consumption was found among 70%, use of fossil fuel was found among 65%, 38% were exposed to poorly ventilated and overcrowded living conditions and 33% were having contact with cattle and animals.
| Districts | Gender | N | Mean BMI |
Std. Deviation | 95% CI for Mean | Min | Max | |
|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||
| Muzaffarabad and Neelum |
Male | 85 | 21.23 | 0.45 | 13.70 | 26.90 | 1 | 4 |
| Female | 45 | 16.55 | 0.56 | 12.76 | 23.59 | 2 | 4 | |
| Poonch | Male | 130 | 20.20 | 0.47 | 12.53 | 25.97 | 1 | 5 |
| Female | 40 | 17.32 | 0.49 | 11.90 | 25.79 | 1 | 5 | |
| Bagh | Male | 465 | 20.11 | 0.61 | 13.89 | 27.74 | 2 | 4 |
| Female | 85 | 16.35 | 0.68 | 12.49 | 24.75 | 2 | 5 | |
| Mirpur | Male | 105 | 21.83 | 0.58 | 14.81 | 27.94 | 2 | 5 |
| Female | 55 | 19.21 | 0.63 | 12.72 | 26.59 | 2 | 5 | |
| Sudhnutti | Male | 67 | 23.00 | 0.39 | 14.67 | 28.21 | 2 | 4 |
| Female | 48 | 18.41 | 0.44 | 12.78 | 25.99 | 1 | 4 | |
| Bhimber | Male | 331 | 22.98 | 0.63 | 13.34 | 27.90 | 2 | 5 |
| Female | 119 | 17.34 | 0.57 | 11.76 | 24.22 | 2 | 5 | |
| Kotli | Male | 86 | 21.54 | 0.54 | 13.10 | 28.23 | 2 | 4 |
| Female | 47 | 16.53 | 0.49 | 11.87 | 24.84 | 1 | 4 | |
| Total | Male | 1269 | 21.70 | 0.68 | 12.53 | 28.2 | 2 | 4 |
| Female | 439 | 17.53 | 0.72 | 11.73 | 26.60 | 2 | 4 | |
3.6. Statistical Analysis
T-test results have shown that the district wise prevalence was not significantly different in 2011 and 2015 with p values = 0.659 and 0.542, respectively (Table 3). There was also no significant difference between male and female prevalence (p = 0.294). However, there was the significant overall decline in tuberculosis infection with (p < 0.01).
4. DISCUSSION
The poverty is largely associated with human health and trend of tuberculosis. Tuberculosis has been a bacterial infection with severe health threats to human populations since the olden times. Mycobacterium tuberculosis attacks the people of lower socioeconomic status because they often face the problems like unhygienic food and crowded living conditions [21-23]. There are reports demonstrating that the population below 40 years of age is the main target of disease in Pakistan [24, 25]. The present study was aimed to monitor the incidence trends of tuberculosis among the underprivileged group of children (orphans) in seven districts of Azad Jammu and Kashmir (Fig. 1). The investigation of 1708 children was carried out to observe any changes in the infection rate during four years (2011 to 2015). The first screening was conducted in 2011 including 733 children and the second study was carried out in 2015 including 975 children (Table 1). Our study has shown 3.41% to 1.95% tuberculosis infection in the years 2011 and 2015, respectively indicating an overall decline in the incidence of disease. The results of our study indicate less prevalence as reported from different areas [26] indicating 6.3% to 6.7% infection, the results also vary from some reports indicating 10% and 15% prevalence in areas of Pakistan and South Africa, respectively [27]. The differences between our results can be described by the fact that the later studies were carried out for the prevalence of TB in association with other diseases like HCV, HBV, HIV and respiratory infections.
However, the present study was conducted on general healthy individuals of a special group of children. The decrease in the prevalence during the 3 years can be associated with an effective role of the national TB control programme, general improvement in the lifestyle of this specific group of children with the support of government and non-government organizations, the availability of funds from the international community after the onset of earthquake in October, 2005. The maximum incidence rate of disease was found in district Bhimber indicating 4.4% and 2% infection in 2011 and 2015, respectively. The lowest rate of infection was found in the Sudhnutti area with 1.66% and 1.81% TB cases in the respective years of investigation. The prevalence of tuberculosis was generally higher among the females as compared to male children. The results correlate with the previous reports from different areas of Pakistan [24, 26]. The mean BMI value for male children was 21.70 (SD±0.68) and that for female children was 17.53 (SD±0.72). On the basis of our findings of the infection rate and BMI, we assume that the higher infection rate among the females is because of less exposure to sunlight and low quality, the unhygienic nutritional status of females in Pakistani society. We have found a little decline in the infection rate regardless of the gender which correlates with the international trends and improvement if living conditions in these areas [28-30]. Our findings of the elevation and decline in blood granulocytes, lymphocytes, PCT, MCV, MCHC, RDW, and plasma calcium are in correlation with the previous studies [31, 32]. The risk factors associated with the disease were also noticed by all the participants.
CONCLUSION
The present study provides a record and tendency of disease frequency in the area often visited by international tourists and media observers. Although a minor decline has been observed in the disease prevalence, yet the findings indicate an alarming situation. These investigations and observations will also help to draw the attention of local health department, national and international public health organizations to contribute to the comprehensive management of health issue of children in the study area. The low BMI suggests nutritional deficiency overall and especially in the female children. We found a clear decline in the tuberculosis infection among orphan children. An alarming situation demands an immediate interference of national and international community.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The study protocols were approved by the Institutional Ethical Committee and Board of Advanced Studies and Research at the University of Azad Jammu and Kashmir Pakistan as notified by the university letter No. F-BASR/ (14th M)/20-73/7060-64/2011.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are bases of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
The authors are grateful to Human Appeal International (HAI), Sector I, Islamabad, Pakistan for the logistic support and conducting screening camps for the children. We are thankful to Higher Education Commission of Pakistan (HEC) for funding this research. We are also very thankful for the participant children who contributed to this study.

