All published articles of this journal are available on ScienceDirect.

Impact of Artificial Intelligence on Healthcare Quality: A Systematic Review and Meta-Analysis
Abstract
Background
Artificial intelligence embodies the ability of computers to emulate human intelligence and generate well-informed choices. Quality within the healthcare domain encompasses adopting proficient, patient-centric, secure, and productive services that are unbiased, comprehensive, punctual, and streamlined. In this regard, this study aimed to investigate the impact of artificial intelligence on healthcare quality. This study echoed the World Health Organization’s findings that artificial intelligence has great potential for distributed clinical automation, delivering efficient clinical information, and offering extra support in healthcare settings.
Methods
This systematic review employed PRISMA methodology and inclusion and exclusion criteria to search through central databases exploring the impact of artificial intelligence on healthcare quality. Specifically, this study concentrated on randomized controlled trials published in PubMed. The search process employed Boolean operators (AND) and (OR) and the main keywords detailed in the methodological section. As a result, two thousand five hundred forty-four sources were identified. The identified sources underwent a rigorous screening process, which entailed the removal of duplication. These eligibility criteria considered studies published in the English language, availability of full text, thorough description of the research aims, objectives, methodology, findings, and conclusion, the number of references, and general presentation. Out of 2544 identified sources, only 18 sources passed the eligibility criteria and were included in this research. The Meta-analysis was conducted using RevMan 5, Mantel-Haenszel, random effect, and 95% confidence intervals.
Results
Overall, the studies were substantially heterogeneous at I2=92%, Z score was 1.93, and the P-value was within the range of less than or equal to 5. Therefore, the general studies provided a significant positive impact of artificial intelligence on healthcare quality. The heterogeneity was minimized through subgroup analysis, where the studies were divided about the objectives. Generally, 6/18 studies yielded an odd ratio of more than 1, reflecting the positive influence of artificial intelligence on healthcare quality. 12/18 studies positively used artificial intelligence in assisted healing or medication adherence, but none were statistically significant.
Conclusion
Artificial intelligence does not directly influence healthcare quality but helps improve other functions within healthcare services. Healthcare quality is comprehensive, encompassing evidence-based practice, patient-centric care, effective communication, care coordination, effective risk management strategies, health information technology, health promotion, and disease prevention.
1. INTRODUCTION
Artificial intelligence is the game-changer across various industries on a global scale, and healthcare is certainly not exempt. Within the realm of healthcare, the pursuit of optimal outcomes necessitates the integration of artificial intelligence. At its core, artificial intelligence embodies the ability of computers to emulate human intelligence and generate well-informed choices [1]. Conversely, quality within the healthcare domain encompasses adopting proficient, patient-centric, secure, and productive services that are unbiased, comprehensive, punctual, and streamlined services [2]. Therefore, the integration of artificial intelligence in healthcare completes the quality equation. Many industries worldwide reckon the enormous benefits and use of artificial intelligence in healthcare. Ideally, prominent health reformers anticipate a future of complete use of artificial intelligence in delivering healthcare services [3]. For instance, the World Health Organization echoes artificial intelligence's potential to perform distributed health automation, give clinical information, and offer extra clinical support [4]. Therefore, this study appreciates that artificial intelligence creates centric and distributed big data hubs that provide informed health information and insights into well-being. Big data is critical in dispensing artificial intelligence in the healthcare industry. The Big data coffers are integrated with machine learning algorithms to diagnose better, identify specific indicators, and inform treatment outcomes [5] on the 20% more polyps than the regular examination [6-8]. AI integrated with machine learning algorithms has a 5% better-improved accuracy and error reduction rate. AI in healthcare potentially reduces medical and operational costs; for instance, a study [9] provided an example of a pill-cam that performed better endoscopy for stomach cancer examinations. Also, a study [10] reported the successful use of AI tools to test acute leukemia, a relatively cheaper exercise than traditional methods. From the dystopian perspective, a question lies on the accountability aspect of artificial intelligence.
For instance, on May 7th, 2016, the Tesla Model S autonomous car encountered a malfunction that led to the demise of a person. Who was accountable for the Tesla Model S accident is a question that can trouble the medical field. Who can account for AI causes of misdiagnosis, failed treatment, or general failure? Nevertheless, the gains surpass the risks, and in this regard, this paper examines the impact of artificial intelligence on healthcare quality.
Despite the growing interest in using artificial intelligence (AI) in healthcare, there is still a lack of comprehensive research on the potential impact of AI on healthcare quality. While some studies have explored the use of AI in healthcare, there is still a need for a systematic review and meta-analysis examining the current state of AI in healthcare and its potential benefits and drawbacks. This study aims to fill this gap by providing a comprehensive analysis of the current state of AI in healthcare and its potential impact on healthcare quality. The findings of this study will provide insights into how AI can be used to improve healthcare quality and inform future research in this area.
1.1. Rationale
The study investigates the impact of artificial intelligence on healthcare quality. In this respect, this study recognizes the revolutionary nature of artificial intelligence in healthcare services. Therefore, the rationale concerns increasing AI integration in healthcare quality, including treatment, diagnostics, planning, and administration. AI growth is on the uptrend; therefore, understanding its impact on healthcare quality is crucial for healthcare professionals, stakeholders, and policymakers. Current AI applications in healthcare showcase its potential in decision-making, especially in data analytics and predictions. AI enhances diagnostic accuracy, efficient resource allocation, and personalized treatment, which significantly implicates the quality of health. However, concerns arise in regulatory frameworks, algorithmic bias, and ethical implications. Therefore, this study explores extensive literature about the impact of artificial intelligence on healthcare quality, providing insights to healthcare providers, stakeholders, and policymakers on future recommendations and current decision-making. The study provides evidence-based information to showcase the impact of AI integration in healthcare.
1.1.1. PICO Research Question
What is the impact of artificial intelligence on healthcare quality?
1.1.1.1. Population (P)
The population of interest in the studies are patients and individuals in diverse demographic groups and with various conditions.
1.1.1.2. Intervention (I)
The utilization and implementation of artificial intelligence in healthcare quality, including administrative processes, treatment planning, predictive analytics, and diagnostic tools.
2. MATERIALS AND METHODS
2.1. Search Strategy
A literature search was conducted from June 5th, 2023, to July 20th, 2023, to identify relevant articles related to the research topic. The search strategy incorporated the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), inclusion, and exclusion criteria [11]. The PRISMA guidelines were imperative for extending the reproducibility and transparency of this review [11]. A PRISMA structural framework is integrated after thoroughly examining the sources through the inclusion and exclusion criteria. Factors considered for inclusion were as follows:
- Language – Only studies published in English were included in this study. It is because highly reputable and impactful journals are published in English. Many researchers use the English language for standardization and call for international collaboration. Also, journals published in English are easy to understand and access.
- Study design- this study majored in Randomized controlled trials (RCTs). RCTs have high internal validity, which reduces bias while helping to control confounding variables in the relationships between the outcomes and the interventions. RCTs offer strong evidence-based practice and help establish the effectiveness of interventions.
- Type of Publications- This study opted for only journal articles published in the PubMed database. Studies from PubMed extensively explore the literature, increasing credible evidence in the generalization. Also, PubMed is user-friendly and standardized. Finally, PubMed has a broad spectrum of biomedical studies.
- Date- Studies published from 2012 and below were excluded. Only studies published in 2012 were included due to their relevance to the issues of artificial intelligence and healthcare quality. The limitation ensures the publications included are relevant to the current and revolutionary topic of study. Therefore, this research addressed notable changes in artificial intelligence and healthcare quality.
An extensive search process incorporated keywords searched using Boolean operators (AND, OR). The operators created a string of variables that simplified the search process, as shown below.
- Artificial intelligence
- Artificial
- Intelligence
- Healthcare
- Quality
- Healthcare Quality
- Artificial intelligence in healthcare
2.2. Critical Appraisal Tools
After the initial screening of the articles based on their titles and abstracts, two reviewers independently evaluated each record for eligibility. The reviewers worked alone and were blinded to each other’s decisions. Any discrepancies between the two reviewers were resolved through discussion and consensus. The inclusion criteria for the systematic review and meta-analysis were based on the research question and were pre-specified in the protocol. The final selection of articles was based on the inclusion criteria and the quality of the studies. Using the PRISMA and Critical Appraisal Skills Programme (CASP) checklists significantly enhanced the quality of this systematic review. The CASP questions were pivotal in meticulously screening the sources before their final inclusion in this review. These questions examined whether the studies appropriately addressed the research question, emphasizing the considered outcome, administered intervention, and targeted population. The primary objective of this review was to ascertain the potential impact of artificial intelligence on healthcare quality. The population under scrutiny consisted of patients undergoing medical treatment after clinical diagnosis and medical chart reviews. Furthermore, randomized trials were considered to analyze the pre and post-effects of artificial intelligence implementation. Consequently, this review diligently verified that participant assignments to interventions were randomized effectively to minimize the likelihood of systematic bias. Additionally, a thorough assessment was conducted to ensure that exclusions and follow-up procedures during and after randomization were adequately accounted for, with careful consideration given to any instances of premature discontinuation of the process. The screening process also considered whether the intervention effects were sufficiently reported, considering the precision of estimates, and whether the experimental intervention considered harms and costs in the entire process. Finally, the transferability and accuracy of the findings were central throughout the screening process.
3. THE PRISMA FRAMEWORK
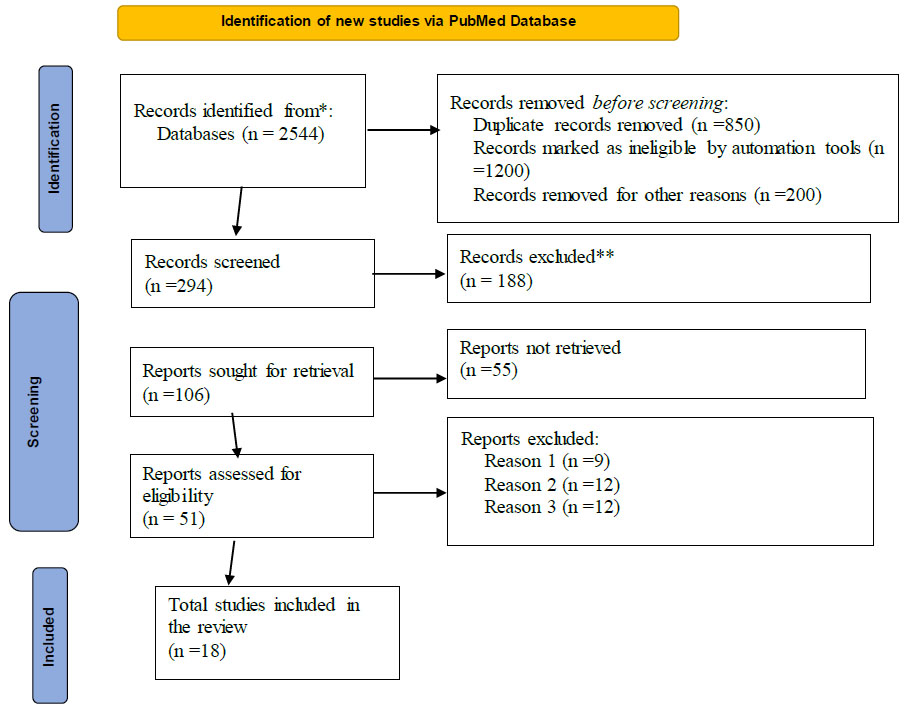
As discussed earlier, this study majored in randomized controlled trials on the impact of artificial intelligence on healthcare quality published in PubMed. As a result, 2544 sources that emphasized the impact of artificial intelligence on healthcare quality were identified. However, 850 sources were duplicates and removed from this study due to irrelevant and inconsistency with this research. Two hundred more records were removed because of insufficient information regarding the topic and methodology. Two hundred ninety-four records qualified for the screening process, whereas 188 sources still needed to meet the year of publication requirements. This study excluded records published from 2012 and below. Moreover, 55 sources were removed since more detailed information concerning the authors was needed. Only 51 records qualified for eligibility, whereas another nine sources failed because they required precise details concerning the intervention and the control groups. Twelve sources were considered close to this topic but slightly different from this research and thus removed. Twelve sources contained mixed research methods, which took more work to follow up on the controls and the intervention groups (Fig. 1). Only 18 sources were included, as shown in the PRISMA flowchart below [7] (Table 1).
| Author(s) and Date | Method | Objectives | n= Sample Size | Control Group | Intervention Group | Results | Implementation |
|---|---|---|---|---|---|---|---|
| 1. Brath H, Morak J, Kästenbauer T, Modre‐Osprian R, Strohner‐Kästenbauer H, Schwarz M, Kort W, Schreier G.2013([2] | Controlled Randomized Crossover design | The aim was to assess mobile health (mHealth) based remote medication adherence measurement system(m A M S) for patients with cardiovascular disease. | 150 | 75 | 53 | The study concluded that mHealth-based medical adherence was well accepted and provided possible results for reduced cardiovascular risk. | The mHealth electronic blisters can be applicable for various medication regimens but need to be examined to establish suitability for their daily applications. |
| 2. Chandler J, Sox L, Kellam K, Feder L, Nemeth L, Treiber F. 2019 [12, 13] | Randomized Controlled Trials | To test the efficacy of real-time monitoring using wireless health technology in controlling blood pressure (BP) and monitoring medication adherence. | 54 | 28 | 26 | The use of real-time smartphone monitoring provided practical solutions for medication adherence and statistically significant results in controlling BP and uncontrolled HTN. | The smartphone-enabled medical regimen can promote medication adherence and significantly reduce SBP in adults with uncontrolled hypertension (HTN). |
| 3. Goldstein CM, Gathright EC, Dolansky MA, Gunstad J, Sterns A, Redle JD, Josephson R, Hughes JW. 2014 [14] | To test medical adherence using telehealth medication versus pillbox for patients with systolic and diastolic heart failure. | 60 | 30 | 30 | The devices were not significant in determining medical adherence. | Medication adherence reflected good management of patients with no relationship between the alarmed pillbox and the smartphone. | |
| 4. Greer JA, Jacobs JM, Pensak N, Nisotel LE, Fishbein JN, MacDonald JJ, Ream ME, Walsh EA, Buzaglo J, Muzikansky A, Lennes IT.2020 [15] | Randomized Trials | The study tested how smartphone applications enhanced adherence to oral therapy for cancer and symptom management. | 181 | 90 | 91 | Smartphone mobile applications did not provide improved medical adherence, and there were no perceptions of quality of care, QoL, and symptoms compared to standard care alone. | Mobile apps can reinforce the bidirectional communication between clinicians and patients in the overall administration of oral cancer therapy. |
| 5. Santo K, Singleton A, Rogers K, Thiagalingam A, Chalmers J, Chow CK, Redfern J.2019 [16] | Randomized control groups | To test the feasibility and effectiveness of the medical apps in improving medication adherence in the control of Coronary Heart Disease. | 163 | 81 | 82 | There was no significant clinical evidence in the Coronary Heart Disease Study that medical adherence apps could improve medication adherence. | Even though the medical reminder apps improved medication adherence, they did not significantly improve different outcomes. |
| 6. Johnston N, Bodegard J, Jerström S, Åkesson J, Brorsson H, Alfredsson J, Albertsson PA, Karlsson JE, Varenhorst C.2016 [17] | Randomized trials | The study examined whether smartphone applications improved treatment adherence and cardiovascular lifestyle in myocardial infarction (MI)patients | 174 | 86 | 80 | The results were not statistically significant that the smartphone application improved treatment adherence and cardiovascular lifestyle in MI patients. | An interactive tool can offer support and provide promising results in collaboration with a secondary prevention procedure. |
| 7. Kim JY, Wineinger NE, Steinhubl SR.2016 [18] | Randomized Control Trials | The study examined how wireless self-monitoring program influenced blood pressure levels, medication adherence, and health behaviors | 95 | 43 | 52 | The wireless self-monitoring program did not provide significant results concerning medicine adherence but strengthened campaigns to reduce alcohol and drug consumption. | Self-monitoring wireless programs motivated the patients to improve their health management and change their health behaviors. |
| 8. Labovitz DL, Shafner L, Reyes Gil M, Virmani D, Hanina A.2017 [19] | Randomized parallel trials | The study tested the implication of AI integrated into mobile devices in increasing medical adherence for stroke patients undergoing anticoagulation therapy. | 29 | 13 | 15 | There was a 67% absolute improvement for patients monitored by the AI app based on the drug levels. | The consistent use of AI applications can optimize medical adherence for patients taking 3DOACs (dabigatran, rivaroxaban, and apixaban). |
| 9. Marquez Contreras, E., Marquez Rivero, S., Rodriguez Garcia, E., López-García-Ramos, L., Carlos Pastoriza Vilas, J., Baldonedo Suarez, A., Gracia Diez, C., Gil Guillen, V., Martell Claros, N. and Compliance Group of Spanish Society of Hypertension (SEH-LELHA), 2019 [20]. | Randomized Controlled Trial | The study investigated the effectiveness of pharmacological therapeutic adherence through a mobile application in controlling mild to moderate arterial hypertension (AHT) | 148 | 77 | 77 | The mobile app intervention favored pharmacological therapeutic adherence for hypertensive patients. | The mobile application improves and requires less effort for pharmacological therapeutic adherence for hypertensive patients. |
| 10. Thimabut N, Yotnuengnit P, Charoenlimprasert J, Sillapachai T, Hirano S, Saitoh E, Piravej K. 2022 [21] | Randomized Controlled Trial | The study investigated using a RAGT (Robot-Assisted Gait Training) device to improve ambulatory functions in Subacute stroke with hemiplegia. | 26 | 13 | 12 | The group that received robotic training showed more significant improvement. | The use of robotic training physiotherapy provided more significant improvement in sub-acute stroke with hemiplegia patients. |
| 11. Sconza C, Negrini F, Di Matteo B, Borboni A, Boccia G, Petrikonis I, Stankevičius E, Casale R. 2021 [22] | Randomized Controlled Crossover Trial | The study tested the effectiveness of robot-assisted gait training (RAGT) in patients affected by multiple sclerosis (MS) and undergoing physiotherapy treatment. | 19 | 9 | 8 | The patients improved their gait parameters significantly after the RAGT training. | Robot-assisted training with physiotherapy gives positive results for patients with multiple sclerosis (MS). |
| 12. Jayakumar P, Moore MG, Furlough KA, Uhler LM, Andrawis JP, Koenig KM, Aksan N, Rathouz PJ, Bozic KJ. 2021 [23] | Randomized Clinical Trials | To test whether AI-enabled patients improve process-level outcomes, functional outcomes, patient experiences, and decision quality. | 129 | 69 | 60 | The AI-enabled platform significantly improved process-level outcomes and decision quality. | Using a data-driven decision-making approach is essential for the management of Knee Osteoarthritis. |
| 13. Yao X, Rushlow DR, Inselman JW, McCoy RG, Thacher TD, Behnken EM, Bernard ME, Rosas SL, Akfaly A, Misra A, Molling PE. 2021 [24] | Randomized Control trials | The study examined whether AI-powered electrocardiogram (ECG) can support the diagnosis of EF. | 22,641 | 11,068 | 11,573 | The AI-powered ECG increased the diagnosis of EF. | AI-powered algorithms in ECG tests can be helpful for EF diagnosis. |
| 14. Adly, A.S., Adly, M.S. and Adly, A.S., 2021 [25] | Single-blinded randomized clinical trials | The use of a Telemanagement health care system compared to two nonpharmacological respiratory treatment methods for COVID-19 home-isolated patients. | 60 | 30 | 30 | There was a significant difference between the control group and the intervention group. | Home-based oxygen therapy provided a prophylactic treatment approach compared to physical therapy and osteopathic manipulative techniques. |
| 15. Rodgers H, Bosomworth H, Krebs HI, van Wijck F, Howel D, Wilson N, Aird L, Alvarado N, Andole S, Cohen DL, Dawson J.2019 [26] | To assess the effectiveness of robotic gym-assisted training for upper limb therapy (EULT). | 770 | 516 | 254 | No improvement of upper limb function after stroke was observed after the robotic gym training. | Robotic gym training does not enhance upper limb function after a stroke. | |
| 16. Seol HY, Shrestha P, Muth JF, Wi CI, Sohn S, Ryu E, Park M, Ihrke K, Moon S, King K, Wheeler P.2021 [27] | Stratified Randomization design | To assess the efficacy of an AI-assisted CDS tool, Asthma-Guidance and Prediction System (A-GPS) for asthma management. | 184 | 94 | 90 | Using AI-assisted and GPS systems can improve the efficiency of clinical reviews in asthma management. | The use of care, the GPS-based intervention, and the AI intervention provided similar results for asthma management. |
| 17. Wilson PM, Ramar P, Philpot LM, Soleimani J, Ebbert JO, Storlie CB, Morgan AA, Schaeferle GM, Asai SW, Herasevich V, Pickering [BW.2023 [28] | Cluster randomized trials | To test the effectiveness of the machine learning decision tools and artificial intelligence tools in predicting patients requiring palliative care services. | 2544 | 1332 | 1212 | Using machine learning decision tools and artificial intelligence provided a higher incidence of palliative care consultation than usual care. | Decision support tools and models can increase palliative care consultation in hospitalized patients. |
| 18. Mori Y, Wang P, Løberg M, Misawa M, Repici A, Spadaccini M, Correale L, Antonelli G, Yu H, Gong D, Ishiyama M. 2023 [29] | Randomized controlled trials | To test whether polyp detection can be increased using artificial intelligence during colonoscopy, | 5796 | 2894 | 2902 | AI increases the detection rate and the proportion of patients requiring intensive colonoscopies. | AI tools may improve cancer detection and prevention, reducing the disease’s cost and burden. |
3.1. Meta-Analysis
This section statistically combines the results of the systematic analysis above to derive conclusions that inform about the topic of this research. Mainly, this research derives from randomized controlled clinical trials about the impact of artificial intelligence on healthcare quality, and this section quantifies the results in the form of forest plots, funnel plots, and risk analysis tables.
3.2. Forest Plots
The general forest plots of the studies in the systematic analysis are shown below:
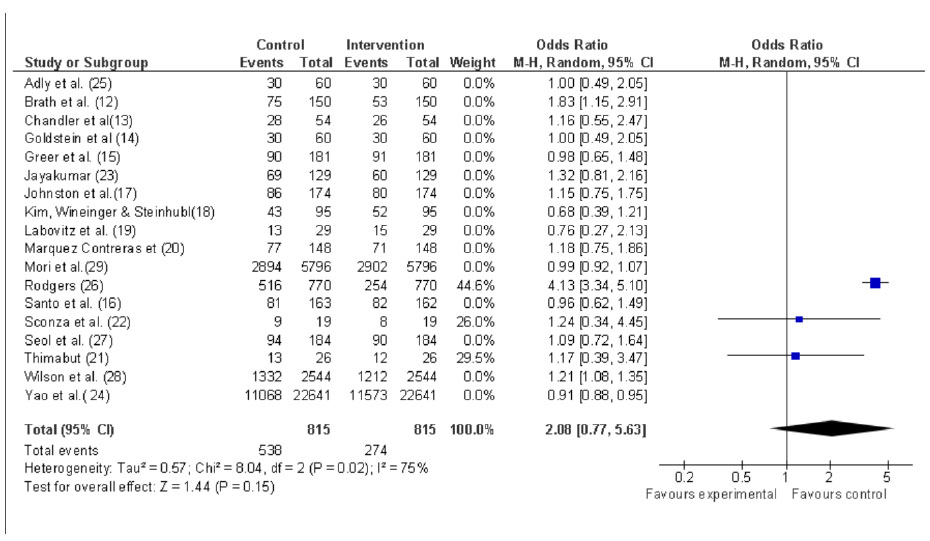
Each line represents the study, and the box shows the estimate’s midpoint; in this research, the box symbolizes the odd ratio. The size of the box represents the weight of the study, which is relative to the N in each study. The larger the sample size of each study, the greater the weight and the bigger the box in the forest plot. For instance, studies by Yao X et al. [24] and Mori Y et al. [29] carry the most significant weight in the study. Fig. (2) is a forest plot indicating the results of the intervention review. The forest plot represents the study labels, the effect size estimates, confidence intervals, the diamond marker, the vertical line of no effect, and heterogeneity statistics. The odd ratios (ORs) show the relationship between the variables in the outcome. It represents the odds of the event occurring versus the control group. 9 out of 18 studies have an odds ratio greater than 1. Odd ratio >1, which indicates there is a significant influence of artificial intelligence on healthcare quality. Therefore, the studies [12, 13, 17, 20-22, 26-28,] prove there is a positive impact of artificial intelligence in healthcare quality. An odd ratio equals 1, indicating no association between artificial intelligence and healthcare quality. In this respect, 2 out of 18 studies showed no relationship between artificial intelligence and healthcare quality. The control group provided results equal to those of the intervention groups. An odd ratio of less than 1 indicates reduced odds of the event occurring. In this regard, 6 out of 18 studies showed decreased odds of artificial intelligence impacting healthcare quality. The studies [15, 18, 19, 29, 16, 24] provided reduced odds of artificial intelligence impacting quality in healthcare.
Heterogeneity measures inconsistency or the degree of variability among the studies. Heterogeneity is represented by I2 statistic and as a percentage. The forest plot figure above shows I2 = 92%, representing considerable heterogeneity, indicating high variation among the studies. The overall effect value indicates Z= 1.93 and P= 0.05; Z-score is used to test the summary measure's statistical significance or effect size. The Z-score shows several standard deviations from the null hypothesis in an observed effect size. Z scores depend on the alpha level in explaining the level of significance where the P-value is considered less than or equal to 0.05. About Fig. (2) above, the Z score is 1.93, indicating a statistically positive significant direction of the effect size observed towards the alternative hypothesis. The null hypothesis is that artificial intelligence does not impact healthcare quality, whereas the alternative view is that artificial intelligence affects healthcare quality. Therefore, this study proves that artificial intelligence positively impacts healthcare quality.
3.3. Funnel Plots
A funnel plot is a scatterplot showing intervention estimates effects against the size of each study. The funnel plots show how the precision of the intervention increases relative to the study size. The effect estimate of studies with small sample sizes scatter at the bottom of the funnel plot. In this regard, this study shows an inverted funnel, indicating the absence of publication bias. Most studies are distributed on the top, meaning extensive studies with no publication bias (Fig. 3).
3.4. Subgroup Analysis
The following section of subgroup analysis is divided in response to the research objectives. The objectives mention using AI mobile technology, AI robotics in healthcare delivery, and AI gadgets in healthcare monitoring. The subgroup analyses are intended to reduce the heterogeneity observed in the general research.
To explore the use of AI integration in mobile technology and its impact on the quality of health.
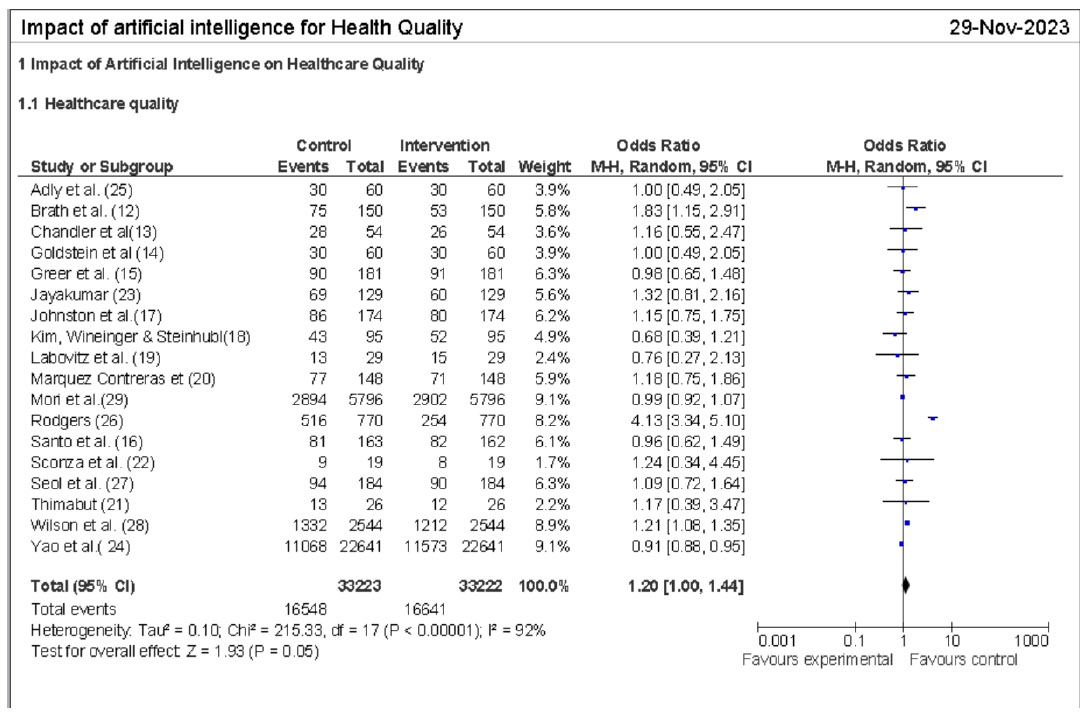
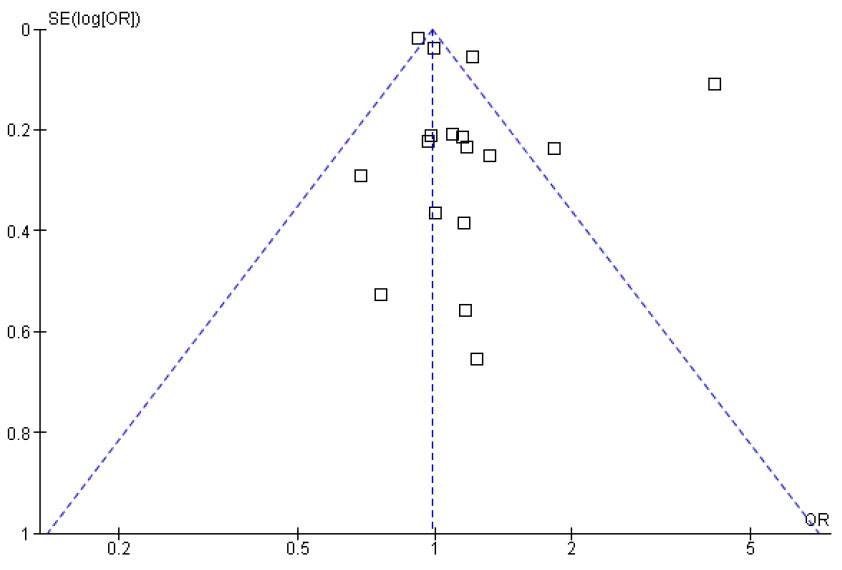
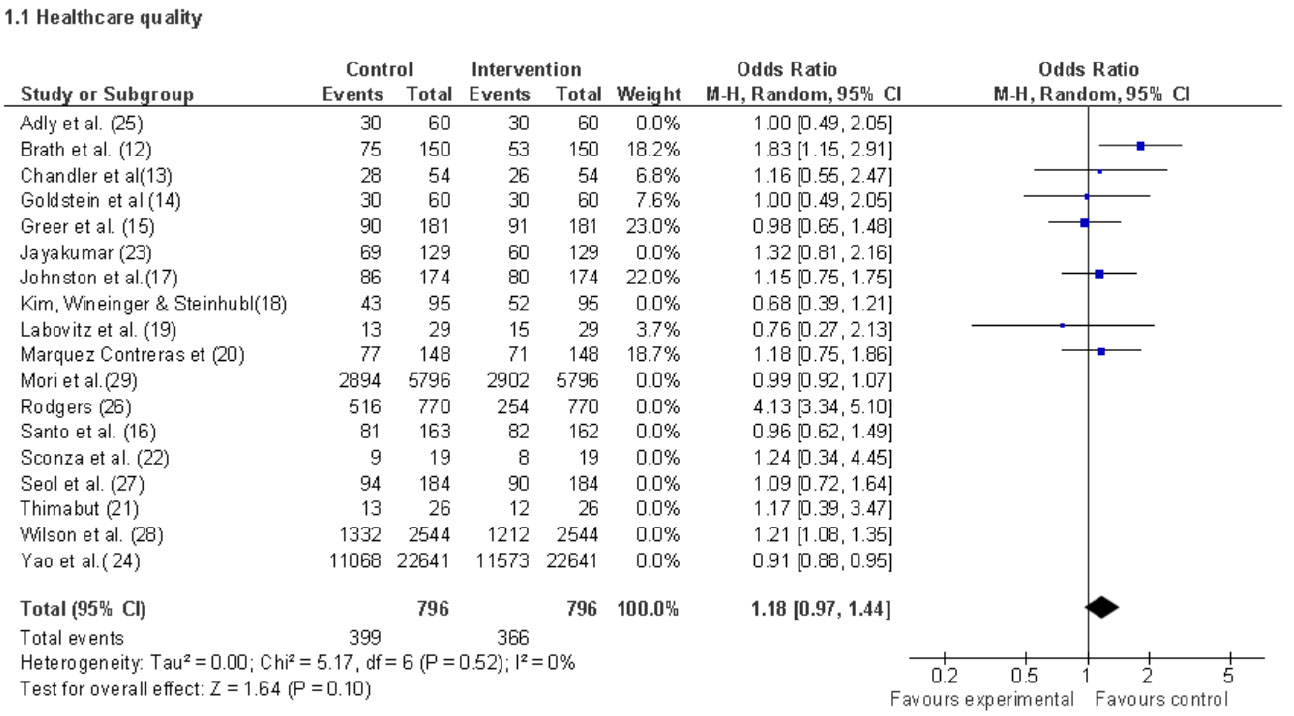
Figure I2 = 0%, which shows that studies relating to AI-enabled mobile technology applications are consistent (Fig. 4). Three of the seven studies showed a lesser positive relationship between AI-enabled mobile technology producing positive healthcare quality. 4 out of 7 studies prove the positive relationship between AI-enabled mobile technology and achieving healthcare quality. A Z score of 1.64 indicates that AI-enabled mobile technologies contribute to positive results in establishing healthcare quality. The studies [12-15, 17, 19, 20] expounded on the use of AI, such as mobile health electronic blisters, to monitor medication adherence in diabetes patients. The electronic blisters provided positive results and can be applied in promoting various medicine adherence regimens [12]. The use of mHealth medication regimens to encourage a culture of self-management for hypertensive patients provided positive results [13]. The use of telemedicine medication reminders to promote medication adherence for older patients with heart failure [14]. However, the telemedicine medication reminders did not provide significant results concerning medication adherence. Mobile smartphone applications were used to help patients with cancer improve adherence to oral therapy [15]. The study observed no perception of care compared to the usual care for cancer patients. Interactive smartphone applications were used to help myocardial infarction patients with drug adherence and lifestyle changes [17]. The results were not statistically significant because interactive smartphone applications help drug adherence for myocardial infarction. They reduce the risk of no commitment of patients undergoing anticoagulation therapy using artificial intelligence [19] and smartphone applications to help hypertensive patients with medication adherence. It can be concluded that AI-powered mHealth applications, smartphone applications, and machine learning algorithms can help hypertensive and cancer patients’ self-management. Nevertheless, the applications do not provide significant results regarding medication adherence. The control and the intervention provided almost similar results. Therefore, artificial intelligence can help improve healthcare self-management processes but does not reflect on the overall quality of healthcare services.
3.5. To Examine the Impact of Robotic-assisted Healthcare on the Quality of Health
Fig. (5) below shows that I2 = 75%, which is considerable, but given the few studies, it arises from the different sample sizes. The Z score of 1.44 with a P-value less than 0.05 indicates that AI-enabled robotics positively affect healthcare quality. All the studies have a positive odd ratio, meaning that AI robotics-assisted healthcare is transitioning to quality healthcare. Other studies majored in AI for assistive healing. For instance, a study [21] sought to improve the ambulatory functions of patients with sub-acute stroke using a robot-assisted gait training device. An author [22] investigated the impact of robotic-assisted training for multiple sclerosis patients. An author [26] examined the impact of robotic-assisted training on stroke patients with upper limbs.
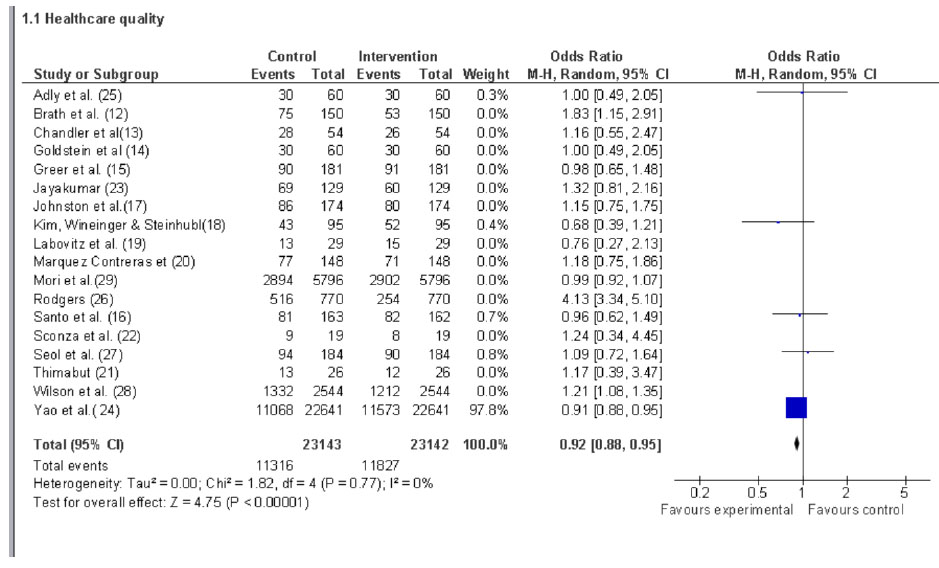
3.6. To Determine the Impact of AI Self-monitoring Hospital Gadgets on the Quality of Health
The I2 = 0 shows no heterogeneity among the selected studies on AI self-monitoring hospital gadgets. Generally, all the studies provided a Z score of 4.75 and a P-value of 0.00001, indicating a positive relationship between AI-enabled self-monitoring healthcare and enhancing quality of health. However, the odds of positive influence varied significantly among the studies. A study [24] investigated electrocardiograms powered by artificial intelligence to help diagnose low ejection fraction. A study [23] compared the performance of the standard educational materials and artificial intelligence-enabled decision-making for patients with knee osteoarthritis. A study [25] investigated the use of Telemanagement for COVID-19-isolated patients in noninvasive oxygen therapy versus the everyday therapy routines. A study [27] investigated artificial intelligence decision-making for asthma management. In contrast, a study [28] investigated the capacity of AI to improve palliative care for hospitalized patients, and another study [29] investigated the use of artificial intelligence for colonoscopy, which provided more polyp than the conventional process. (Fig. 6).
The studies using artificial intelligence for assistive healing are highly heterogeneous, and the p-value significantly influences the results, indicating the presence of publication bias. Generally, all the studies have proven the use of artificial intelligence in healthcare settings as an assistive tool in the diagnosis, treatment, management, and predictability of diseases. Therefore, artificial intelligence requires a combination of other factors in healthcare settings to provide the anticipated healthcare quality.
4. RESULTS AND DISCUSSION
This study confirms the effectiveness of artificial intelligence in improving healthcare processes, especially in assisted healing and medication adherence. For instance, a study [12] examined the use of mHealth for remote medication adherence, and the study confirmed the widespread acceptance of the device. Examples of mHealth mobile devices include tablet computers, smartphones, and personal digital assistants [7]. Healthcare professionals use tablet computers and smartphones for communication and computing, simplifying the point-of-care processes [30, 31]. Moreover, artificial intelligence provides expanded functionalities such as sound recorders, high-quality cameras, global positioning systems (GPS), web searching powered high-resolution screens, significant memories, and robust operating systems promoting exceptional services and deliveries [7]. However, a study [12] cautioned the need to examine the devices to gauge their applicability and suitability in daily applications. According to a study [6], smartphones provide adequate support for caregivers and remote workers in health services. However, the study [6] argues that smartphones face financial, technical, security, and communication constraints that may hinder the delivery of the intended benefits. Therefore, the study [6] confirms the need to employ cautionary measures as provided [12]. Such functionality is exceptional in providing real-time monitoring, which is significant in controlling lifestyle diseases such as blood pressure [23]. Real-time health monitoring devices improve the quality of life by helping patients maintain independence, preventing complications, and minimizing personal costs [32]. In addition, real-time monitoring helps extend quality care in the comfort of patients' homes [8]. The capacity of real-time monitoring health devices to monitor and predict trends helps reduce emergency visits and hospitalization. It improves patients’ psychological parameters, which helps in improving the quality of healthcare services [8]. However, the study [14] did not observe statistically significant results of telehealth services versus a pillbox in managing patients with systolic and diastolic heart failure. Similarly, the study [15] did not observe any advantage of using smartphone applications in assisting cancer patients in maintaining oral therapy. A Study [16] also confirms that the medical reminder apps do not significantly improve medication adherence, which is similar to findings postulated by other studies [17, 18, 26]. Generally, the studies showcased the benefits of artificial intelligence integrated into computer and smartphone technologies in diagnosis and healing processes in healthcare settings. For instance, a study [19] observed that AI applications could optimize medical adherence for patients taking 3DOACs (dabigatran, rivaroxaban, and apixaban). A Study [20] Observed the effectiveness of mobile applications in pharmacological therapeutic adherence for hypertensive patients. AI-based technologies have significantly transformed the healthcare sector, particularly disease diagnosis and treatment, encompassing a wide spectrum of medical conditions [33]. The advantages are particularly pronounced in the context of real-time automatic detection for cancer patients [34]. The amalgamation of AI and machine learning algorithms confers a multifactorial capacity that enables precise and comprehensive cancer diagnosis [35]. This progress has facilitated the accessibility of sophisticated healthcare services for diagnosing and managing complex diseases in rural regions through AI-assisted diagnosis, prediction, and treatment [36]. Nevertheless, implementing AI-assisted technologies in clinical settings presents various challenges: financial considerations, hardware utilization, security concerns, and communication issues. Despite these obstacles, mobile devices provide healthcare professionals with precise and actionable functionalities, significantly enhancing time and information management capabilities [7]. The application of AI in managing acute leukemia has yielded remarkable outcomes, as advanced diagnostic methods now provide highly categorized information [37]. They showcased the benefits of artificial intelligence integrated into computer and smartphone technologies in diagnosis and healing processes in healthcare settings.A study [21] showcased the effectiveness of robot-assisted gait training for sub-acute stroke patients.A study [22] observed the advantages of robot-assisted gait training for multiple sclerosis (MS) patients. A study [29] observed that AI diagnosis improves polyp detection rate in colonoscopy. Ideally, robotic technology offers many advantages in improving healthcare quality. Robotics can perform accurate and precise tasks that reduce the risk of human errors [38]. Also, robots operate using predefined guidelines and protocols that ensure standardization and consistency, reducing variability and improving quality [9]. Ideally, robotic-assisted surgeries are less invasive due to the smaller incisions resulting in reduced pain, faster recoveries, and fewer complications [10]. In addition, AI-powered robotics help surgeons discover or access difficult areas that increase precision while reducing complications [39]. AI robotic technology provides greater access in underserved and remote regions to treat and monitor patients remotely, reducing the need to travel [9].
The limitations of this systematic review and meta-analysis include the search strategy. It is not comprehensive enough to identify all relevant studies, as the search was conducted on one PubMed database. This may have resulted in missing some relevant studies published in other databases or not indexed in PubMed. This limitation could have been addressed by searching multiple databases and using different sources such as reference lists of included studies and grey literature.
The results suggest that artificial intelligence has a positive influence on healthcare quality. However, the studies were substantially heterogeneous, which may limit the generalizability of the results. The lack of statistical significance in 12/18 studies may be due to the small sample sizes or the lack of standardization in using artificial intelligence in healthcare. The positive influence of artificial intelligence on healthcare quality suggests that it may be helpful in assisted healing or medication adherence. Future research should focus on standardizing the use of artificial intelligence in healthcare and increasing sample sizes to improve the generalizability of the results. Additionally, future research should investigate the potential adverse effects of artificial intelligence on healthcare quality and patient outcomes. The implications of these results for practice and policy suggest that artificial intelligence may be helpful in improving healthcare quality and patient outcomes. However, more research is needed to determine the optimal use of artificial intelligence in healthcare and to ensure that it is used ethically and responsibly.
CONCLUSION
The utilization of artificial intelligence (AI) enhanced by machine learning algorithms and integrated into mobile technologies and applications was consistently observed throughout the studies. However, none of the studies demonstrated statistically significant evidence that AI directly improves healthcare quality. This study uncovers the multifaceted factors contributing to enhancing healthcare quality, such as ensuring individuals have access to timely healthcare services, including emergency care, specialists, and primary care. Furthermore, prioritizing the patient’s values, preferences, and needs in healthcare decision-making can improve patient satisfaction and outcomes. Effective communication, evidence-based practice, and care coordination are other factors that can help enhance healthcare quality. Finally, incorporating health information technology, safety, and risk management can help proactively respond to adverse events and minimize hospital errors, thus improving healthcare quality.

