All published articles of this journal are available on ScienceDirect.

Enhancing Clinical Data Quality to Improve Patient Care in Rural Health Facilities
Abstract
WHO recognizes that high-quality research is not just a scientific pursuit but a crucial factor in achieving global health, health equity, and economic development. It is not just about the numbers but about the lives we can save and improve. In this context, four research priority areas have been identified: prioritizing health needs, building research capacity, ensuring good research practice, and ensuring good evidence is translated into practice. Local health research tailored to local needs remains an important global health goal, with the potential to revolutionize patient care in rural health facilities.
Researchers and policymakers in low- and middle-income countries have expressed serious concerns about the limited access to high-quality data, a fundamental requirement for reliable and valid research. The assessment of data quality is typically categorized into five key areas: availability, usability, dependability, relevance, and presentation quality. This concept is further clarified by demonstrating how a robust healthcare data environment can enhance patient management through research efforts. The term ‘health data environment' encompasses the entire process of gathering, storing, managing, analysing, and utilizing health-related data to improve patient care and healthcare policies through informed decision-making. In this context, we present the challenges that undermine the quality of research data and propose solutions. Specifically, we identify the lack of adequate human resources, reliance on paper-based records systems, and the high costs of internet connectivity as the primary barriers to collecting and sharing high-quality data for research in low-resource settings. To tackle these challenges, we advocate for governments and funding institutions to invest in data management and communication systems, recruit and train data management staff to support clinicians, and reduce connectivity costs. Furthermore, we propose the deployment of a decentralized system as a cost-effective and less labor-intensive solution that only requires data entry staff at health facilities in resource-limited settings.
This article explores current data collection, storage, and interpretation challenges and proposes innovative improvement solutions. It emphasizes the transformative potential of digitization, standardization, and staff training to enhance data quality. It further addresses the impact of quality data on evidence-based practice, ultimately leading to improved health outcomes. Focusing on rural healthcare facilities sheds light on the unique barriers these settings face, proposing tailored strategies that can bridge the gap between urban and rural health service delivery. These insights offer valuable guidance for policymakers, healthcare administrators, and practitioners striving to improve patient care in rural areas through data-driven strategies.
1. BACKGROUND
The World Health Organization (WHO) regards high-quality research as one of the most important factors in achieving global health, health equity, and economic development [1]. To that end, four research priority areas have been identified: prioritizing health needs, building research capacity, ensuring good research practice, and ensuring good evidence is translated into practice. Local health research adapted to local contexts remains an important global health goal [1].
Over the last ten years, quality research output in Low and Middle Income Countries (LMICs) has increased significantly [2]. While the growing research output is a significant improvement, it should be noted that it is currently concentrated in well-established institutions in low-income countries with established funding and research infrastructure [2]. Pan et al. reported on making regional collaborations for evidence synthesis in Africa, naming well-established African institutions as the leading players in evidence synthesis publications. This motivates us to seek ways to strengthen research capacity equitably, including in underserved regions in Africa. Clinical research capabilities and data archiving must be strengthened in resource-constrained settings to achieve the global health agenda.
The importance of reliable and accurate clinical data cannot be overstated in the evolving healthcare landscape. This data forms the backbone of evidence-based practice and is pivotal in patient diagnosis, treatment, and overall care. However, in rural health facilities, clinical data quality often suffers due to many factors, including resource constraints, lack of trained personnel, and inadequate infrastructure, as highlighted by O’Neill and colleagues [3]. The disparity in clinical data quality between urban and rural healthcare facilities further exacerbates existing health inequities. In rural settings, where access to healthcare services is already limited, the implications of poor-quality data can be dire, leading to sub-optimal patient outcomes.
While there have been considerable advancements in health information technology, these are often not effectively implemented in rural areas due to infrastructural and financial constraints. As a result, rural health facilities often struggle to maintain the accuracy and reliability of clinical data, which is crucial for improving patient care.
This study focuses on these critical issues, providing an in-depth examination of the challenges faced by rural health facilities in maintaining high-quality clinical data. It also explores potential strategies for enhancing data quality, aiming to provide a roadmap for improving patient care in these underserved areas.
1.1. Operational Challenges
Researchers in low- and middle-income countries have lamented the lack of access to high-quality data [3]. A systematic meta-narrative review identified barriers to research capacity building in LMICs, such as fragmented research systems, where different components, such as clinical and laboratory databases, are not linked, insufficient funding for reliable health record systems, and a lack of dedicated personnel with the necessary research skills, among other aspects [4].
A shortage of clinicians and healthcare professionals is an important barrier to quality data collection and research in resource-limited settings. Clinicians in these settings often perform dual functions as data entry clerks; hence, data collection tends to get overlooked in favour of the pressing healthcare-related roles. The amount of time required for accurate patient data collection has been studied; physicians spend 35% of their time recording patient data, and ironically, even more time if electronic health record systems are used [5]. As such, unless the dynamics of data collection change, the research agenda in LMICs is unlikely to advance. Understanding the local context and accurately assessing existing research and data collection capacity are two key recommendations for improving research output in LMICs, particularly in resource-constrained settings [3].
For research to be accurate and valid, high-quality data is required. According to Cai and Zhu [6], data quality metrics can be broadly classified into availability, usability, reliability, relevance, and presentation quality. This is further explained by Jarwar MA and Chong, who illustrated how data quality within the healthcare domain could improve patients’ management through research activities, as shown in Fig. (1) [7].
Another barrier to collecting good-quality data in LMIC is the use of paper-based records. There is a paucity of data documenting the progress in transitioning from paper-based records to HER in LMIC countries. However, much progress has been made in high-income countries [8]. In resource-constrained communities, most records related to patient care and related processes are paper-based and handwritten. Large amounts of patient data are lost due to insufficient and inadequate storage and archiving. Records are entrusted to patients in some areas to improve communication within the health system. This haphazard storage system also jeopardizes patient privacy and opens the door to medicolegal cases due to unauthorized access to the records. In South Africa, rising medicolegal costs threaten funding basic medical services, resulting in a vicious cycle of deteriorating healthcare quality and additional litigation. Inadequate recording and unauthorized access to records contribute to the loss of potentially defensible cases. The usability, reusability, reliability, and readability of handwritten, unstructured paper-based records are major concerns. The inability to archive information is hampered by a lack of structure. These deficiencies significantly impact data quality and integrity for research purposes, making secondary data analysis and retrospective studies difficult.
Databases and secondary data are an inexpensive way to answer specific research questions or lay the groundwork for future work. However, these databases need significant input to set up. There are numerous advantages to using secondary data, including expanding available information for various research questions, faster research progress without the time required for data collection, access to larger sample sizes for rare events, and the possibility of longitudinal observation. However, the accumulation of data volumes in the form of databases and secondary data remains a challenge. Deploying and maintaining electronic databases and associated personnel is generally unaffordable to the already struggling health facilities, which default to a flawed paper-based records system. Where a decent body of data has been accumulated, clinical researchers sometimes find it difficult to design research questions that fit the available data.
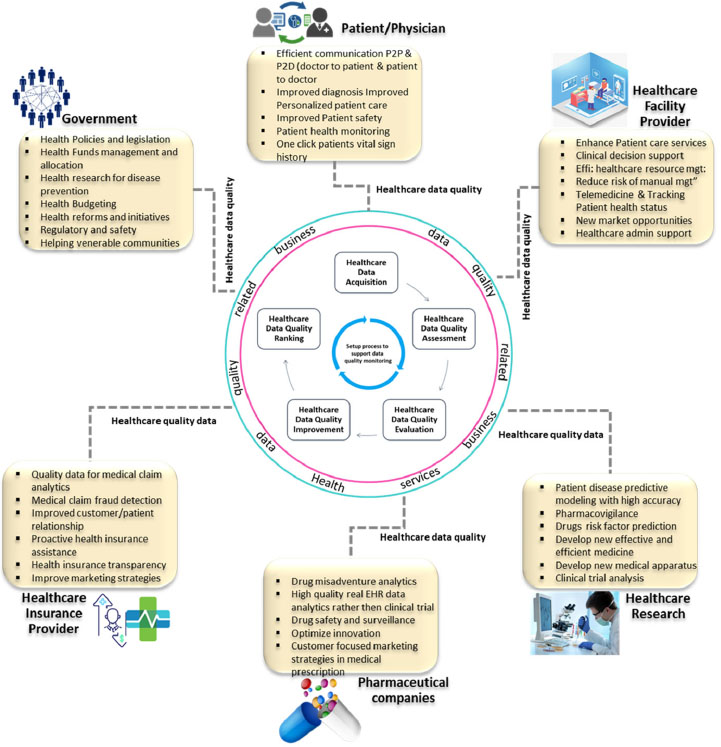
Data quality importance and application in healthcare for improved patient management. Available online under the terms and conditions of the creative common Attribution (CC-BY 4.0) License (CC-BY 4.0) (https://creativecommons.org/licenses/by/4.0/legalcode) [7].
Additionally, South Africa's internet access prices are globally competitive but fall short on download speeds and value for money. Given the lower GDP per capita allocation, these prices make internet access unaffordable for many potential researchers in resource-constrained settings. Xu and Reed reported a link between research output and country internet penetration [9]. The importance of connectivity in many practical aspects of experimental science, such as monitoring and precisely controlling the experimental conditions, is also supported by evidence from laboratory research [10].
These primarily revolve around collecting, managing, and utilizing high-quality clinical data in rural health facilities.
The first challenge is the lack of resources, which can hinder the effective collection and storage of clinical data. These constraints often stem from the limited financial capacity and infrastructural inadequacies common in rural areas.
Second, there is a dearth of trained personnel to manage and interpret clinical data accurately. This can lead to data errors, affecting the reliability of the information and, ultimately, patient care.
Third, the absence of efficient digital systems for data management presents a significant challenge. While health information technology has advanced rapidly, these advancements are not always effectively incorporated in rural settings.
Finally, disparities between rural and urban healthcare facilities can exacerbate health inequities. The challenge lies in bridging these gaps to ensure that high-quality clinical data can be used to improve patient outcomes regardless of the geographical location of healthcare facilities.
1.2. Implementable Strategies
Several solutions can be implemented to enhance the quality of clinical data and improve patient care in rural health facilities.
Adequate funding and resources should be allocated to develop robust data collection, storage, and management systems, including hardware, software, and networking capabilities.
Regular training programs should be conducted for healthcare staff on the importance of clinical data, proper data entry, and interpretation practices. This would also involve training personnel to utilize digital systems for data management.
Standardized data collection and reporting protocols should be established to ensure consistency and accuracy. These protocols should be easy to understand and follow for all healthcare personnel.
Health information technology solutions, such as Electronic Health Records (EHRs) and telemedicine, should be utilized. These technologies can improve the efficiency and accuracy of data collection and facilitate better coordination of care.
Regularly monitoring and evaluating the data quality and patient outcomes are other significant measures. This can help identify improvement areas and ensure the effectiveness of implemented solutions.
Policy changes prioritizing enhancing clinical data quality in rural health facilities should be advocated. This could involve lobbying for increased funding, better infrastructure, and training programs.
1.3. Practical Solutions
1.3.1. Transform From Paper-based Systems to Electronic Health Records
An electronic health record (EHR) is viable. Its main benefits are medicolegal privacy, national and international research, collaboration, and monitoring for improved care quality. Furthermore, although not always possible, EHR connections with other systems, such as imaging and laboratory systems, add value and are desirable for patient care efficiency. Deployed at the national level, a decentralized system, such as the DHIS2, reduces the maintenance cost for local organizations and supports the integration of datasets from various sources. Additionally, it provides a universal framework to address the known pitfalls of electronic health records, such as structure, data precision, and user interface. Furthermore, data entry clerks must be recruited and adequately trained to lift the burden of data entry from the already under-resourced clinical personnel. This, in turn, will provide reliable data for research and other purposes and help ensure its completeness, accuracy, and timeliness.
1.3.2. Enhance the Quality of Internet Connectivity
The main measure is to deploy a decentralized system, such as DHIS2, to reduce the cost of Internet connectivity. Recent advances have allowed the proliferation of 4G and LTE wireless technologies that support high-speed connections at relatively affordable costs, making it possible to invest in dependable internet as part of building research capacity. This, however, will necessitate collaboration between the government, international funding bodies, and the private sector, including network company sponsorships aimed at hospitals, universities, and research hubs. Even with the most reliable connection, however, internet down times remain a challenge. Significant progress has been made in developing software that allows data collection and storage without the use of the internet, such as the RedCap and other electronic data-capturing platforms designed to ensure the success of the proposed model.
1.3.3. Develop Human Capability
Human capacity, including data collectors as needed, should be focused on relieving the patient care workload. Another role that must be considered in the planning is data monitoring and continuous maintenance of the EHR. Biostatistician capacity has previously been identified as one of Africa's recommended research capacity-building focus areas [11].
CONCLUSION
We have illuminated several limiting factors to accumulating high-quality research data in clinical settings and proposed solutions to these challenges. We have particularly emphasised the role of a decentralized electronic health system. The rollout would require a reliable internet connection and dedicated staff to capture and analyse data. The presented findings will be crucial in supporting the public health response and planning. Research opportunities to be explored in this area should include the impact of improved data management on patient-centered outcomes and detailed cost analysis of investments in good quality data for improved health outcomes. Such an analysis should explore metrics like mortality, hospital utilisation, and medicolegal costs.
AUTHORS’ CONTRIBUTION
B.M. and O.O.: Conceptualized the idea, wrote the first draft, and edited the manuscript. Both authors read and approved the final version.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| LMICs | = Middle Income Countries |
| EHRs | = Electronic Health Records |

