All published articles of this journal are available on ScienceDirect.

Raising Awareness on The Impacts of Caesarean Section Birth Method to Children's Health: Nationwide Survey to Indonesian Married Woman
Authors Info & Affiliations
Abstract
Aims
This study seeks to determine the level of knowledge mothers have about CS and its health implications, such as gut dysbiosis, before and after a health promotion.
Methods
We analyze the awareness of Indonesian mothers through a cross-sectional survey before and after health promotion, utilizing digital health education through national parenting platforms, PrimaKu and TemanBumil.
Findings
A total of 769 participants completed both the pre-test and post-test. There is an increase of awareness (70% to 95%), total score (mean ± SD: 4.34 ± 0.99 to 4.83 ± 0.49; p-value 0.000), and correct answer for each question (p-value < 0.05), respectively from pre-test and post-test. Instagram posts (77.07%), webinar (38.9%), Instagram live (35.94%), and Tiktok videos (34.02%) are the most preferred to least preferred forms of content, respectively.
Conclusion
Digital health campaigns using social media and webinars had a beneficial impact on raising awareness among Indonesian mothers about the impact of CS on children's health.
1. INTRODUCTION
Cesarean section (CS) is a procedure of fetal delivery involving an abdominal incision (laparotomy) and uterine incision (hysterotomy) [1]. CS deliveries increased over time globally; they were 5% in 1970, 15.3% in 1991, and 31.7% in 2012, despite the fact that less than 10% of all deliveries had a medical reason. It is believed that the majority of the increase in cesarean section rates is due to medical indication whether from the mother or their fetuses, alongside an increase in elective cesarean sections [2]. In Indonesia, the rate of cesarean section increased from 9.8% in 2013 [3] to 17.6% in 2018. [4]
C-Section is a life-saving procedure for both mother and child [5], but there is limited understanding among pregnant women and/or mothers on the health impact of C-Section to children [6], not excluding in Indonesia. Increasing awareness on this topic can help achieve the third Sustainable Development Goals (good health and well-being), especially target 3.2 to End all preventable deaths under 5 years of age and target 3.7 for Universal access to sexual and reproductive care, family planning, and education. Women have the right to be informed and educated on their and their children’s health, hence, this study contributes to the literature on C-Section health impact perspectives among married women in the Indonesian landscape, which is currently still quite limited [7]. According to a recent survey in a low-middle-income country, around 78% of pregnant women were unaware that a CS may have negative effects on the infant [6]. Children born through CS have a higher risk of developing asthma, respiratory tract infection, atopy, allergy, and cognitive impairment, however there is a lack of awareness and comprehension regarding this issue [8-11]. There is also a correlation between method of delivery with initial breastfeeding and skin-to-skin contact between mother and infant. Mothers who delivered through CS are 7.16 times more likely than those who deliver normally to delay lactation [12]. Vaginal delivery is associated with 4.8 times the likelihood of skin-to-skin contact than cesarean delivery [13].
The colony of intestinal microbes differs between babies born through CS and those delivered vaginally. The bacteria colony in CS babies has less normal microbiota and has a different colony than healthy individuals in the community, a condition known as dysbiosis [10, 14-16]. Dysbiosis reduces the development of immunity in children and increases the risk of other conditions and diseases associated with cesarean section [15].
A systematic review revealed that infants delivered through caesarean have less Bifidobacterium and Bacteroides colonization and more Clostridium, Lactobacillus, Enterobacter, Enterococcus, and Staphylococcus colonization [17]. Another study reveals a decline in Bifidobacterium and Enterobacteriaceae, as well as an increase in Clostridium, in infants born via CS [10]. Bifidobacterium is one of the essential microbiotas that plays a significant role in protection, including against respiratory tract infections [16], and is less commonly found in infants with allergies [10]. Early life is a crucial phase, during which the infant's immune system is still developing and is affected by the gut microbiota; hence, any dysbiosis caused by environmental variables such as mode of delivery or antibiotic administration may result in enduring health consequences [18]. Hence, it is imperative that gut dysbiosis in C-section children be treated as early as possible to prevent health problems, especially in the immune system. Breastfeeding is the primary treatment for a baby with gut dysbiosis. The alternatives to breastfeeding include breast milk donors, breast milk fortifiers, infant formula feeding with specific fatty acid supplementation, vaginal seeding, microbial environment, prebiotic, probiotic, and synbiotic supplements [19, 20]. Synbiotic supplementation may improve the intestinal tract environment and its normal microbiota more identical to their physiological state, thereby decreasing dysbiosis-related conditions/diseases in infants born through cesarean section [18, 21, 22].
Due to the lack of awareness and knowledge, it is crucial to intervene early on this topic, for example through health promotion. Health promotion, a form of primary prevention, can be utilized to raise public awareness of the negative health effects of CS on children. There are a variety of tools available, notably through the utilization of online parenting communities. Another study from Indonesia about health promotion for CS are scarce, in our findings, there is one study about the development of a digital application for application-based education about CS [23], however, no study about health promotion effect on child health and CS. In April, in commemoration of CS Awareness Month, we conduct a health promotion and campaign about the effect of CS on child health, such as dysbiosis, and the role of breastfeeding or other nutritional intake to optimize the child’s health. This study seeks to determine the level of knowledge mothers have about CS and its health implications, such as gut dysbiosis, before and after a health promotion.
2. MATERIALS AND METHODS
During the “Caesarean Section Awareness Month” campaign in Indonesia, this cross-sectional pre and post-test survey was utilized as an evaluation instrument. The campaign was facilitated by national parenting platforms in Indonesia that are credible and trusted by experts/ pediatricians. We collaborate with PrimaKu and TemanBumil on this campaign. TemanBumil and PrimaKu were selected as these platforms are some of the biggest digital parenting communities in Indonesia to reach a wider audience and optimize impact. They are also known for their credibility through their close collaboration with pediatric experts. The campaign is conducted via an online webinar held on April 5th 2023 (TemanBumil) and May 26th 2023 (PrimaKu), with a focus on the child health of CS born children. The webinars consist of an expert (pediatrician subspecialized in gastro-hepatology or allergic immunology) presentation, followed by an interactive discussion with the participants. Participants were asked to fill in the pre-survey before the webinar and the post-survey after the webinar. Participants were reached through PrimaKu and TemanBumil’s audience and community of parents, who are exposed to banners and flyers inviting them to attend the event. As the main objective is health promotion to raise awareness of Indonesian married women, participants are free to join with little to no further requirements. Additionally, the PrimaKu campaign includes in-app articles, Instagram posts, Instagram live, and Tiktok videos.
The target population consists of married women, pregnant women with or without children, and/or expectant mothers. The population members who attended the campaign and responded to the pre-test and post-test questionnaires constitute the study sample. Google Form is used to incorporate the survey into an electronic format. The question is written in Bahasa Indonesia and has been reviewed by a subspecialist pediatrician in the relevant field. It consists of five questions with two possible answers, one of which is correct and the other incorrect. The questions are presented in the supplementary materials. Each correctly answered question is worth 20 points, for a total of 100. In addition to the five questions, we collect demographic information about the women (such as pregnancy status), whether they have or do not have a child, and residing city. The pre-test and post-test questionnaires are available in the supplementary materials.
Participants were not required to execute a written consent form, as consent was implied by their registration. The campaign and questionnaire are accessible using the participant's own device. Before joining the session, participants must register and complete a pre-assessment questionnaire. Participants were requested to complete the post-test questionnaire after the discussion. Google form was utilized to compile the survey responses. The ethical clearance had been approved by the ethical committee of Universitas Muhammadiyah Purwokerto with registration number KEPK/UMP/12/V/2024 and following the Helsinki Declaration.
The compiled responses were further statistically analyzed using SPSS software. Using descriptive analysis, we evaluate each question's correct response before and after the health promotion. The cumulative score of the five questions was then statistically analyzed using the paired t-test and descriptive analysis before and after health promotion.
3. RESULTS
There was a difference in the number of participants who responded to the pre-test and post-test. Individuals who responded to both the pre-test and post-test are included in the data set. Seven hundred sixty-nine participants are further analyzed derived from Teman Bumil (N=706) and PrimaKu (N=217) as shown in Fig. (1). Five questions were evaluated for their validity, and each was found to be valid.
Among the respondents, 433 (56.3%) of the 769 participants are not pregnant and already have offspring, 136 (17.7%) are pregnant and have offspring, 170 (22.1%) are pregnant, 11 (1.4%) are pregnant and without offspring, 11 (1.4%) are on a pregnancy program, and 8 (1%) are not pregnant. Our participants originate from 20 out of 38 provinces in Indonesia. Most participants live in West Java (28.47%). The demographic characteristic of respondents is shown in Table 1
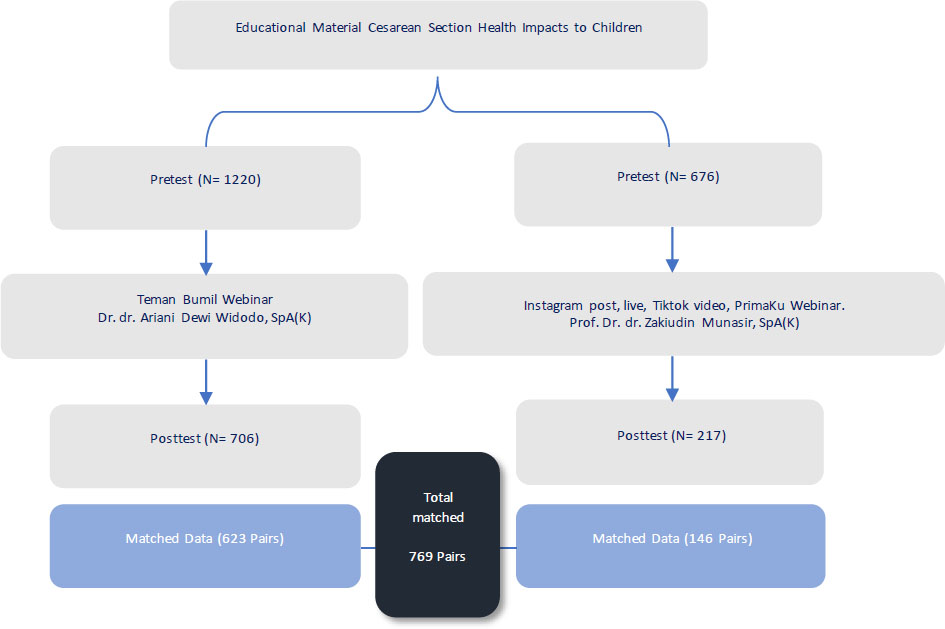
Method of campaign.
| Province | - | |
|---|---|---|
| n | % | |
| Aceh | 2 | 0.26% |
| Bali | 6 | 0.78% |
| Banten | 70 | 9.10% |
| Bengkulu | 3 | 0.39% |
| DKI Jakarta | 111 | 14.43% |
| Jambi | 1 | 0.13% |
| West Java | 219 | 28.47% |
| Central Java | 79 | 10.27% |
| East Java | 149 | 19.37% |
| South Kalimantan | 9 | 1.17% |
| Central Kalimantan | 1 | 0.13% |
| East Kalimantan | 5 | 0.65% |
| North Kalimantan | 1 | 0.13% |
| Riau Islands | 4 | 0.52% |
| Bangka Belitung Islands | 1 | 0.13% |
| Lampung | 7 | 0.91% |
| East Nusa Tenggara | 3 | 0.39% |
| Papua | 1 | 0.13% |
| Riau | 13 | 1.69% |
| South Sulawesi | 8 | 1.04% |
| North Sulawesi | 1 | 0.13% |
| West Sumatera | 13 | 1.69% |
| South Sumatera | 14 | 1.82% |
| North Sumatera | 11 | 1.43% |
| Yogyakarta | 37 | 4.81% |
| Respondent’s pregnancy status | ||
| Not pregnant and already have offspring | 433 | 56.3% |
| Pregnant and have offspring | 136 | 17.7% |
| Pregnant and without offspring | 11 | 1.4% |
| On pregnancy program | 11 | 1.4% |
| Not pregnant | 8 | 1% |
Based on the score of the analysis of the pre-test, the question with the fewest correct responses is question number 1, with 31.7% incorrect responses, and the question with the most correct responses is question number 2, with only 3.0% incorrect responses. This trend changes with the intervention of the post-test questionnaire answer, with number 3 becoming the most incorrectly responded (5.7) and number 2 remaining the most correctly answered with a false proportion of 0.9%. Before and after the intervention, each question showed an improvement with a significant p-value. The description of each question's score is provided in Table 2 and Fig. (2).
| Question | N (%) | Question | N (%) | p – value* |
|---|---|---|---|---|
| Pre Q1 | 525 (68.3%) | Post Q1 | 727 (94.5%) | 0.000 |
| Pre Q2 | 746 (97%) | Post Q2 | 762 (99.1%) | 0.001 |
| Pre Q3 | 644 (83.7%) | Post Q3 | 725 (94.3%) | 0.000 |
| Pre Q4 | 708 (92.1%) | Post Q4 | 748 (97.3%) | 0.000 |
| Pre Q5 | 718 (93.4%) | Post Q5 | 755 (98.2%) | 0.000 |
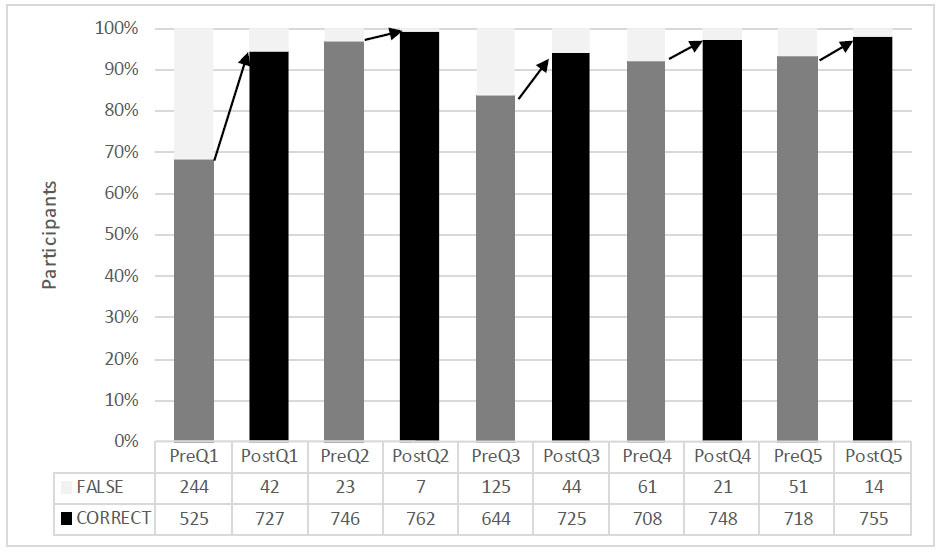
Participants’ answers.
Table 3 displays the wide range of total pre-test scores: 0 correct responses [n = 5 (0.7%)], 1 correct response [n = 13 (1.7%)], 2 correct responses [n = 26 (3.4%)], 3 correct responses [n = 84 (10.9%)], 4 correct responses [n = 181 (23.5%)], and 5 correct responses [n = 460 (59.8%)]. Based on the post-test total score, there was no respondent with 0 correct response, 1 respondent (0.1%) with one correct response, five respondents (0.7%) with two correct responses, twenty-one respondents (2.7%) with three correct responses, sixty-seven respondents (8.7%) with four correct responses, and six hundred seventy-five respondents (87.8%) with five correct responses. The mean ± standard deviation of total scores on pre-test and post-test are 4.34 ± 0.99 and 4.83 ± 0.49, respectively. Based on the total score, 36 subjects scored lower with 1 or 2 incorrect responses in the post-test compared to the pre-test, while the remaining 733 subjects scored the same or higher. Four out of five individuals with zero correct answers on the pre-test answered all post-test questions accurately. Statistical analysis with a paired t-test of the pre-test and post-test reveals a significant (p=0.000) increase between the pre-test and post-tests. The analysis of the total score is shown in Table 4.
| - | Correct Answer | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | |
| Pretest, n (%) | 5 (0,7%) | 13 (1.7%) | 26 (3.4%) | 84 (10.9%) | 181 (23.5%) | 460 (59.8%) |
| Posttest, n (%) | 0 (0%) | 1 (0.1%) | 5 (0.7%) | 21 (2.7%) | 67 (8.7%) | 675 (87.8%) |
| Posttest PrimaKu, n (%) | 0 (0%) | 0 (0%) | 1 (0.6%) | 2 (1.3%) | 12 (8.2%) | 131 (89.7%) |
| Posttest TemanBumil, n (%) | 0 (0%) | 1 (0.1%) | 4 (0.6%) | 19 (3.0%) | 55 (8.8%) | 544 (87.3%) |
| - | Mean | Standard Deviation | P-value* |
|---|---|---|---|
| Total Pretest | 4.34 | 0.99 | 0.000 |
| Total Posttest | 4.83 | 0.49 |
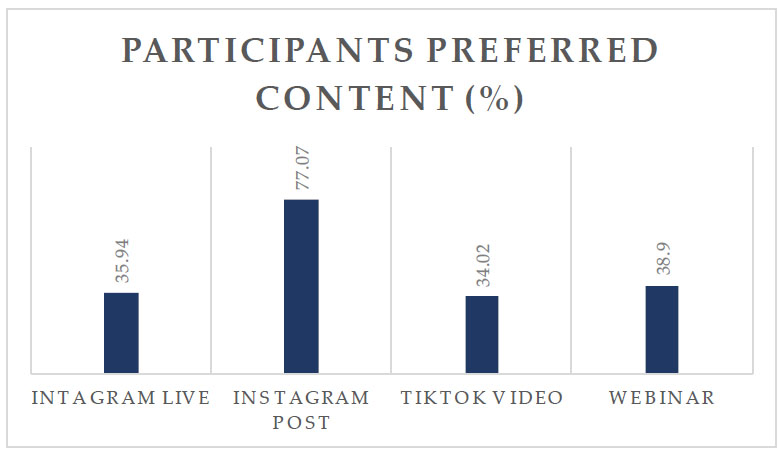
Participants’ preferred content.
Seventy percent of the 1,893 respondents to the pre-test survey are cognizant of the impact of pregnancy methods on the health of their children. After the intervention, the same question was conducted and improved results. Ninety-five percent of the 769 users who responded to the post-test survey are aware of the impact of pregnancy methods on the health of their children. These total results were comprised of the PrimaKu campaign (75 to 95%) and the TemanBumil campaign (67 to 95%) from the pre-test and post-test survey, respectively.
We queried participant preferences between Instagram live, Instagram posts, TikTok videos, and webinars collected from the pre-test survey, where each individual could select multiple options. Instagram post (77,07%) is the most popular content, followed by webinar (38,9%), Instagram live (35,94%), and Tiktok videos (34,02%) shown in Fig. (3).
4. DISCUSSION
The majority of our participants originate from urban areas in Java Island, particularly Jakarta, West Java, East Java, and Central Java. There are few participants from rural areas or from outside of Java. A study conducted in Tanzania from 2000 to 2013 regarding sociodemographic factors of CS revealed a greater number of CS in urban areas, where the odds of having a CS increased by 6%, compared to rural areas, where the odds increased by 3%. They also discovered that the likelihood of a CS increases when the father has a lower degree of education, whether he lives in the city or the country [24]. Another study on the demographics of CS in Indonesia found that mothers from urban areas are more likely to have CS than mothers from rural areas; in contrast with the study from Tanzania, mothers in Indonesia with formal education are more likely to have CS than those with no formal education; and mothers from wealthy families are more likely to have CS than those from low-income families [25].
According to the pre-test survey analysis, our study participants favored Instagram posts the most, followed by webinars, Instagram live, and Tiktok videos, in that order. The majority of respondents selected Instagram posts (image) over the other option (video). The most common formats used for digital health education are images, messages, brief messages, and videos, in descending order of frequency. In the meantime, video has the highest rate of positive outcomes [26]. Facebook and YouTube were utilized as intervention instruments to modify health-related behavior more frequently. Meanwhile, more people used Twitter and Instagram to track the trend of altering health behavior [27].
During the campaign, a greater number of individuals completed the pre-test than the post-test. We recommend including a small number of different questions between the pre-test and post-test, as well as using a more distinct caption or flyer when distributing the questionnaire to participants to prevent them from mistaking them for the same survey.
Each question's specifics are presented in the supplementary materials. The question with the lowest number of right answers on the pre-test is number 1, where only 68.3% of respondents responded correctly to the question “Did you know the difference between CS delivered children and vaginally delivered children?” This implies that in accordance with the limited literature available, participants are not aware of the different gut microbiota colonization between CS-born children and vaginal born children. Hence, it is necessary to raise awareness on the topic for a wider audience, such as what was done in this project.
The question with the correct answers is number 2 in both the pre-test and post-test, garnering up to 97% correct responses in the pre-test and 99.1% in the post-test. This shows that respondents understood that gut health plays an important role in children’s health, especially their immune system. With 70-80% of the immune system in the gut, making the gut our largest immune organ [28], it is imperative to ensure a child has healthy gut microbiota and good gut health. An optimal immune system will protect the child against viral and bacterial pathogenic as well as adapt and bring tolerance to food-related antigens [29].
It is interesting to note that after the intervention, the post-test question with the fewest right answers changes to number 3. In continuation with the first question, CS-delivered children do not get beneficial microbes from the birth canal and are therefore at risk of developing gut dysbiosis. Regarding the third question, “What is the definition of gut dysbiosis?” gut dysbiosis refers to the imbalance of microbes in the children’s gut, which is more pathogenic than beneficial microbes. There is also a correlation between children's immunity, cognitive function, and gut dysbiosis, which poses a potential problem. Through the Hypothalamus-Pituitary Axis, metabolites, vagal nerve, myelination, and neurotransmitters, gut dysbiosis may diminish children's cognitive function and immunity [30-33]. Although question 3 received the least number of correct responses on the post-test, it still received 94.3% correct responses, which is already a significant increase (p=0.000) compared to the pretest, which achieves 83.7% correct answers. Regardless, each question demonstrated a significant (p-value < 0.05) increase in correct participant responses.
Most respondents answered correctly for questions numbers 4 and 5 both in pre-test and post-test. It is implied that respondents have understood that synbiotics in breastmilk are beneficial for their CS born babies because the synbiotic in breastmilk restores the microbial balance in the gut (question 4). It is also suggested that respondents are also aware of the definition of synbiotic (question 5), which is a combination of live microorganisms that, when administered in adequate amounts, confer a health benefit on the host (probiotic) and the substrate that is selectively utilized by host microorganisms conferring a health benefit (prebiotic). For easier understanding among respondents (who are laypeople), a probiotic is simplified as “beneficial bacteria” and prebiotic as “food for beneficial bacteria.” [34-36]
Our study determined that a digital health campaign is beneficial for increasing mothers' awareness and understanding of Caesarean delivery and its effects on mother and child. A recent systematic review of digital health campaign/education about pregnancy during the prenatal period revealed significant participant outcomes, including knowledge increase, affective benefit, and behavioral change [26]. Nonetheless, the effect may be adjusted for low-income pregnant women and mothers of small children due to the low level of participation in digital health campaigns [37].
Another way to prevent post-natal gut dysbiosis during pregnancy is by taking into account maternal diet and nutrition. Maternal consumption of a high-fat diet leads to a reduction in the diversity of gut microbiota. Therefore, it is advisable for mothers to consume a sufficient amount of dietary fat. Administering probiotics to mothers also yields favourable results. During pregnancy, folic acid is given to support the neurodevelopment of the newborn, which happens through the breakdown of one-carbon metabolism [38].
There are a few limitations in this study. The post-test is administered a relatively brief time after the intervention; therefore, our study cannot assess the efficacy after a longer period of time, the participants' memory retention, or whether this influences the participants' delivery method preference. Although we received a significant number of subjects, the majority are from urban areas. Indonesia's vast array of sociodemographic factors may necessitate additional research involving subjects from a larger rural area or outside Java. Future research on the topic may incorporate various study methods beyond cross-sectional method for stronger results and implications. The utilization of novel techniques in the healthcare field, such as Artificial Intelligence (AI), can also help in health promotion to increase awareness of the impact of C-Section on children’s health. Other than that, more research beyond awareness or knowledge increase can be done to observe whether there is a change in attitude and/or behaviour of C-Section mothers’ future pregnancies. Further study to assess awareness can include confounding variables as demographic data to minimize bias and analyze more subgroups.
CONCLUSION
Digital health campaign commemorating CS awareness month with social media and webinar has a positive impact on participants' knowledge of the impact of CS on children's health, as measured by an increase in questionnaire scores before and after intervention. Participants' preferred method of consuming content is through Instagram posts. The majority of participants are from urban areas with higher levels of sociodemographic factors than rural areas. Further studies are recommended to reach out to more participants and more confounding variables. This study contributes to the literature on C-Section health impact perspectives among mothers in the Indonesian landscape, which is currently still quite limited.
AUTHORS’ CONTRIBUTION
The authors confirm their contribution to the paper as follows: FD, CD; draft manuscript: EK, MSK, RWB. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CS | = Cesarean section |
| AI | = Artificial Intelligence |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical review and approval were approved by ethical committee of Universitas Muhammadiyah Purwokerto, Indonesia, with registration number KEPK/UMP/12/V/2024.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this research are available within the article.

