All published articles of this journal are available on ScienceDirect.

Examining Economic Development and Health Outcomes: A Comparative Analysis of BRICS and Non-BRICS African Countries
Authors Info & Affiliations
Abstract
Introduction
Life expectancy has steadily increased worldwide due to advancements in healthcare, improved living standards, and innovative public policies. However, there is limited research on how international alliances, such as BRICS membership, influence these improvements, particularly within the diverse socio-economic landscape of Africa. This study compares key health and economic indicators across South Africa (a BRICS member), Nigeria, and Algeria (non-BRICS nations).
Methods
This comparative analysis used data from eight data sets collected between 1991 and 2015. Data was cleaned using Microsoft Excel and analyzed using STATA version 16.
Results
Algeria recorded the highest GNI per capita, closely followed by South Africa, while Nigeria recorded the lowest. Nigeria recorded the highest life expectancy and employment rates, suggesting elements beyond BRICS membership, like population dynamics, determine health outcomes. South Africa reported the highest HIV prevalence, though it has declined over time, underscoring the need for sustained health interventions.
Discussion
The findings suggests that BRICS membership alone does not guarantee improved labor or health outcomes. South Africa's BRICS status did not yield markedly better life expectancy or maternal mortality rates than Nigeria or Algeria. Conversely, Nigeria and Algeria may have accessed alternative international partnerships to enhance income distribution and economic security.
Conclusion
This study highlights the differences between BRICS and non-BRICS African countries, suggesting that while international alliances may support development, comprehensive, multi-sectoral approaches are essential for sustainable progress in health and economic well-being. Results can inform future policy development aimed at enhancing both economic growth and public health in African countries.
1. INTRODUCTION
The BRIC (Brazil, Russia, India, China) is a coalition of countries with prominent emerging economies that first convened in 2006. In December 2010, South Africa, the only African country, was admitted as a member, changing the name to BRICS (Brazil, Russia, India, China, and South Africa) [1-3]. South Africa's membership was an indication that the country was growing economically in terms of GDP growth, per capita income, exports, and imports. South Africa, the only African country considered a prominent emerging economy, can serve as a case study for comparing BRIC countries with other African countries. This affiliation has sparked interest in examining whether BRICS membership provides distinct advantages in socio-economic and health outcomes relative to other African countries.
Life expectancy at birth serves as a comprehensive indicator of a country's overall development and is shaped by an array of socio-economic determinants. Over the last century, life expectancy has improved across the world due to several factors, including reductions in infant mortality, rising living standards, improved lifestyles, better education, and advancements in healthcare and medicine [4-10].
Several studies have examined life expectancy trends and other health-related issues across various African countries [11-14]. A 2016 study examined the impact of HIV/AIDS prevalence on life expectancy in South Africa [15]. Many of these studies were either limited to single-country analysis or did not consider South Africa's unique BRICS affiliation compared to other African nations, such as Nigeria and Algeria, in their analyses. Furthermore, the majority of these studies did not analyze the unique position of BRICS versus non-BRICS contexts within Africa. Existing research frequently investigates the economic impacts of BRICS membership for South Africa, suggesting potential health and economic gains from international partnerships [1, 2]. However, most of these studies do not directly reference life expectancy in their analyses or provide comparative analyses with non-BRICS African countries. There is a need for a clearer understanding of how South Africa's BRICS membership might influence its socio-economic or health outcomes compared to non-BRICS African counterparts.
This study addresses the gaps in these previous studies by comparing life expectancy and related socio-economic indicators in South Africa, Nigeria, and Algeria, assessing whether BRICS membership confers distinct health and economic advantages for South Africa. Specifically, it aims to determine if BRICS membership correlates with improved life expectancy outcomes in ways that may not be as accessible to Nigeria, Africa's most populous country (World Health Organization), or Algeria, the continent's largest country by land area [16, 17]. This comparative framework will provide insights into the implications of BRICS membership on health and economic development within Africa.
Nigeria, a non-BRICS country, was selected for this study due to its status as Africa's most populous country and its diverse socio-economic landscape. Despite having significant natural and human resources, Nigeria faces numerous challenges, including high rates of infant and maternal mortality and economic disparities [17-19]. These issues starkly contrast with South Africa and Algeria, making Nigeria a compelling case for examining the interplay of health and economic factors on life expectancy.
Algeria, another non-BRICS country, was included in this analysis to provide a comparative perspective within the Maghreb region and to highlight the effects of different socio-economic policies on health outcomes [17, 20]. Understanding Algeria's context allows for a nuanced comparison with Nigeria and South Africa, offering insights into how varying health and economic development approaches impact life expectancy across these three countries.
The objective of this study is to compare infant mortality, maternal mortality, HIV prevalence, gross national income (GNI) per capita, employment rates, and life expectancy across three African countries: South Africa, Nigeria, and Algeria.
2. METHODS
Between January and March 2019, eight datasets were retrieved from reputable repositories [21-26]. Only those collected between 1991 and 2015 were included in the analysis. To address the challenge of limited data availability across the selected African countries, information was sourced from multiple reputable repositories. The datasets were imported and cleaned using Microsoft Excel and subsequently analyzed using STATA version 16. Table 1 provides a summary of the sources utilized in this study.
| Variable | Data Source | Measurement / Description |
|---|---|---|
| Life Expectancy | World Bank; WHO Global Health Observatory | Average number of years a newborn is expected to live, based on current mortality rates |
| GNI per Capita | World Bank; Central Bank of Nigeria | GNI adjusted to constant international dollars, per mid-year population |
| Employment Rate | Index Mundi; World Bank | Percentage of working-age population employed, standardized using ILO definitions |
| HIV Prevalence | AVERT (South Africa, Nigeria); WHO | Percent of adults (15-49) living with HIV |
| Infant Mortality | Our World in Data; WHO | Number of infant deaths per 1,000 live births |
| Maternal Mortality | New Internationalist; WHO | Number of maternal deaths per 100,000 live births |
| Health Infrastructure | WHO; Country-level policy reports (content analysis) | To contextualize public health outcomes and system response |
To ensure ethical compliance, each data set was accessed following the organization's respective data usage and privacy policies.
3. RESULTS
Fig. (1) displays employment rates across three nations: Nigeria, South Africa, and Algeria. Nigeria leads with the highest employment rate at 52%, reflecting a robust labor market. South Africa's employment rate is 40%, while Algeria has the lowest rate at 36%. These figures demonstrate varying levels of employment among the countries, providing valuable insights into their economic conditions and workforce participation. Understanding these employment rates is crucial for assessing the labor market dynamics in these regions.
Fig. (2) shows that Algeria recorded the highest GNI per capita at $14,220, followed by South Africa at $12,850, with Nigeria trailing at $5,880 Fig. (2). Algeria's GNI per capita increased the most, followed by South Africa, with Nigeria having the lowest increase.
Fig. (3) presents a graph of HIV prevalence in the three countries. As shown below, the prevalence of the disease is almost non-existent in Algeria but is significantly higher in South Africa. The rate of growth of the disease increased from 1% in 1991 to almost 19% in 2015. Nigeria also recorded a steady rise in prevalence, though a less dramatic trend than South Africa, which increased from 1.4% in 1991 to 3.7% in 2002 and then gradually declined to 2.9%. In Algeria, the prevalence remained consistently low at 0.1% throughout the period under review.
Nigeria recorded the highest infant mortality rate among the countries Fig. (4), but this rate gradually declined over the years, from 125.4 in 1991 to 68.7 in 2015. South Africa's infant mortality rose from 1994 to 2005 (it is worth noting that at this time, they were not yet members of BRICS) and then declined in subsequent years, while Algeria's infant mortality consistently declined. Algeria's infant mortality rate steadily declined from 40.9 to 21.4.
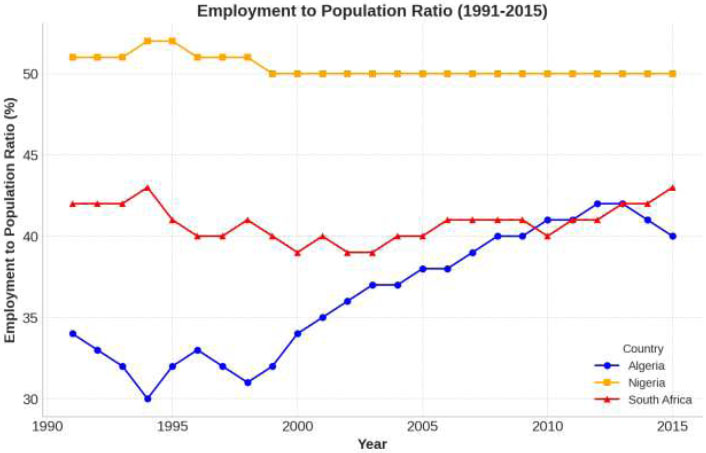
Employment to population ratio in Algeria, Nigeria, and South Africa.
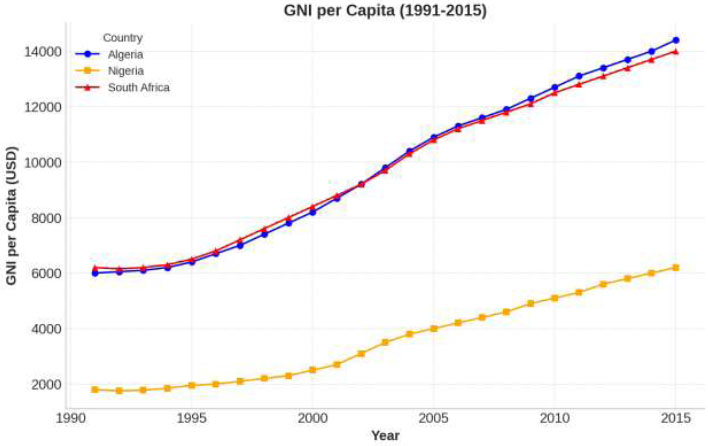
GNI per capita in Algeria, Nigeria and South Africa.
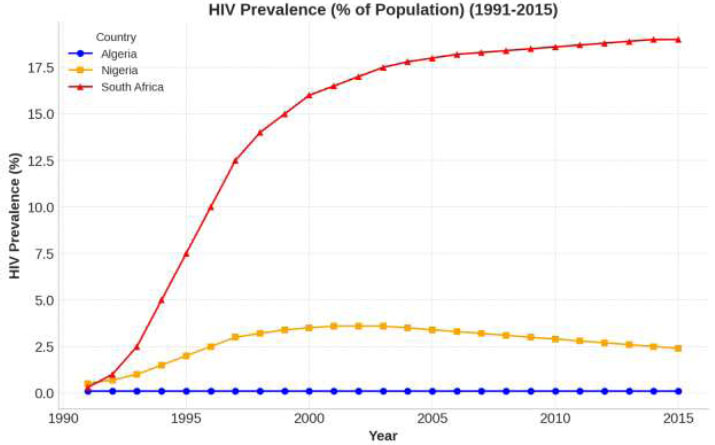
HIV prevalence in Algeria, Nigeria and South Africa.
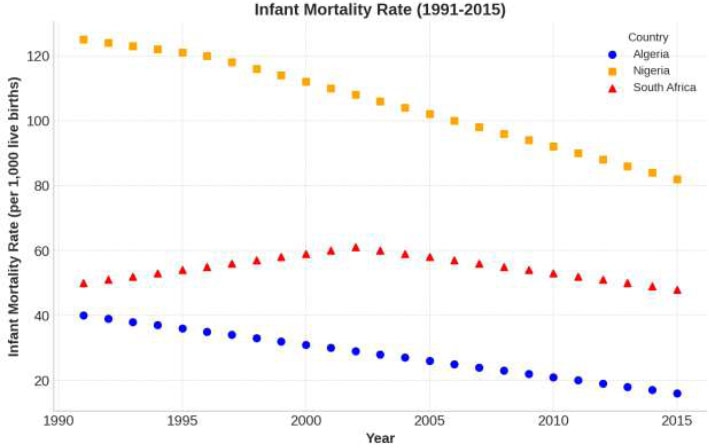
Infant mortality rates in Algeria, Nigeria and South Africa.
Nigeria reported the highest maternal mortality rate, but this rate steadily declined from 1,320 in 1991 to 814 in 2015 Fig. (5). Algeria's maternal mortality rate also showed a steady decline, from 210 per 100,000 in 1991 to 140 in 2015. South Africa, which had the lowest maternal mortality rate in 1991, slowly rose to 138 in 2015. Similar to the trend in infant mortality, maternal mortality in Nigeria, though the highest among the countries under review, recorded a consistent decline. In 2008, the maternal mortality rates for Algeria and South Africa were almost identical.
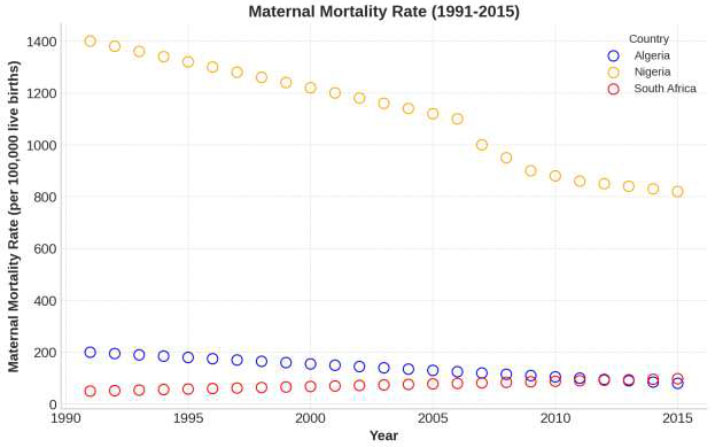
Maternal mortality rates in Algeria, Nigeria and South Africa.
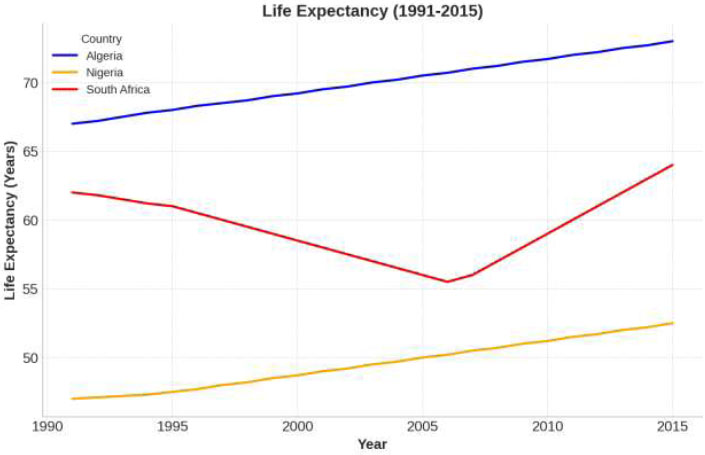
Life expectancy at birth in Algeria, Nigeria, and South Africa.
Fig. (6) shows the difference in life expectancy trends across the three countries. Algeria and Nigeria's life expectancy increased steadily from 1990 to 2016, while South Africa's life expectancy dipped in 1993 and rose again in 2006.
4. DISCUSSION
This comparative analysis of life expectancy, employment rates, gross national income (GNI) per capita, HIV prevalence, infant mortality, and maternal mortality in Nigeria, Algeria, and South Africa offers valuable insights into the socio-economic and public health trends of these three African nations between 1991 and 2015. Each variable examined in this study provides context for how life expectancy trends relate to broader socio-economic determinants in BRICS and non-BRICS countries.
Results suggest that despite South Africa's BRICS membership and the economic partnerships that came with the status has not adequately reflected in the country's employment rate. Throughout the 25-year period studied, the country's employment rate continued to lag behind Nigeria's. This result might be attributable to Nigeria's significantly larger youth population, which has translated to higher labor force participation, a stance supported by previous research [27].
We found that while household income and living standards in South Africa improved overall after the BRICS affiliation, the relatively lower employment ratio indicates that BRICS affiliation did not necessarily result in significantly higher labor market expansion or enhanced life expectancy than in Nigeria and Algeria. Algeria's employment levels remained stable but low, suggesting that a partnership such as BRICS might have stimulated job growth and further stabilized gains in life expectancy in the country.
An interesting finding was that Algeria had the highest GNI per capita of the three countries, closely followed by South Africa, while Nigeria reported the lowest GNI per capita. This is particularly shocking given that previous studies suggest South Africa's affiliation with BRICS has improved the country's per capita income [2, 28]. However, based on this result, the BRICS advantage seems modest. We suggest that Algeria's oil wealth has played a significant role in maintaining a higher GNI per capita despite not being part of BRICS. In contrast, Nigeria's significantly lower GNI per capita highlights the challenges of converting population size and oil wealth into increased per capita wealth. This result suggests that BRICS membership might have provided a country like Nigeria with structured international partnerships to improve income distribution and bolster economic security.
Regarding HIV prevalence, one of the predictors of life expectancy, we found that South Africa's HIV prevalence decreased after 2006. Previous research has linked this decrease in HIV prevalence rate to the extensive health interventions the country has implemented over the years, most of them funded through international partnerships [15, 29]. The rapid rise in HIV rates during the 1990s had significantly impacted life expectancy, so the decline of HIV prevalence also coincided with improvements in life expectancy. The international health partnerships, facilitated by BRICS affiliation, provided vital support, enabling the country to tackle the HIV epidemic more effectively. In contrast, Nigeria and Algeria have maintained more contained HIV rates, with Algeria's remaining negligible throughout the years. This disparity suggests that while association with BRICS can provide much-needed support for addressing critical public health issues such as HIV, it does not replace the need for proactive health initiatives. Nigeria's lower HIV prevalence, despite the lack of benefits from a BRICS affiliation, further supports this notion.
The trends in infant mortality reveal that Nigeria had the highest rate among the three countries, although there was a gradual decline. The infant mortality rate has continued to rise in Nigeria, with any improvements being brief and sporadic. This result could be explained by limited healthcare resources and low government health expenditures in Nigeria between 1970 and 2012 [27, 30]. According to UNICEF, nearly 10% of global newborn deaths occurred in Nigeria in 2016 [18]. The relatively moderate infant mortality rate in South Africa suggests that while the economic resources associated with BRICS positively impacted infant mortality rates and overall health outcomes, there is a need to address other factors that influence life expectancy. Thus, effective governance and healthcare management are still needed to convert economic gains from international partnerships into real, sustainable health advancements. Algeria's consistent decline in infant mortality, despite its lack of BRICS affiliation, further supports this point.
On the other hand, South Africa's maternal mortality rates rose steadily over the years, compared to the sharper declines recorded in Algeria and Nigeria. This result reflects the persistent disparities in healthcare access in South Africa despite BRICS membership and its resulting economic benefits. While the BRICS association afforded South Africa resources to address broader health challenges, the slower progress on maternal mortality rates highlights the challenges of translating economic advantages into targeted healthcare improvements for vulnerable populations. This result contradicts previous research that showed that increased employment rates, GNI, and public health spending lead to improved maternal and child health outcomes. For instance, one study suggests that a decrease in maternal mortality rates can lead to a rapid and sustainable increase in life expectancy (up to 0.6 years) [13, 30, 31]. Future studies could explore targeted interventions to reduce maternal and infant mortality and, by extension, improve life expectancy in these countries.
Overall, the results of this study showed that South Africa's life expectancy trajectory changed over the years. Between 1998 and 2006, South Africa's life expectancy rates decreased. This period also coincides with when the HIV epidemic began in South Africa. Between 2008 and 2010, life expectancy rates improved. It is worth noting that South Africa gained its BRICS status, which boosted international partnerships and health funding, during this time. However, unlike Algeria, which has experienced a consistent increase in life expectancy, South Africa's life expectancy rate remained lower than it was prior to the HIV epidemic (1990 to 1996). This result indicates that BRICS membership did not completely shield the country from all the domestic health issues that negatively affect life expectancy. This comparison highlights the potential relationship between BRICS membership and health outcomes, while emphasizing the urgent need for effective domestic health policy and management.
Algeria, classified as an upper-middle-income country, is the largest nation in terms of land size in Africa and a major oil and gas exporter [32]. This economic power might explain the improved health outcomes, including life expectancy. Algeria's economic resources and focused government spending on public health may have also helped reduce infant and maternal mortality rates, contributing to the steady rise in life expectancy.
Despite being one of Africa's largest oil producers with considerable natural wealth, Nigeria faces numerous challenges. The country struggles with corruption, political instability, and ineffective macroeconomic management, which have impeded its ability to enhance healthcare infrastructure and address high infant and maternal mortality rates [27]. Although Nigeria has since made gradual progress, evidenced by an increase in life expectancy from 54.1 years in 2000 to 63.4 years in 2023, the country still falls short of achieving optimal health outcomes and the projected 70-year life expectancy goal set as part of the Millennium Development Goals [16, 23, 33, 34].
Given these results, we have observed that while BRICS affiliation offers significant economic gains that can translate to better health outcomes, other vital factors determine the GNI, maternal mortality, infant mortality, and life expectancy of the countries examined in this study.
5. LIMITATIONS
While this study provides valuable insights into factors related to life expectancy in BRICS and non-BRICS countries in Africa, it has several limitations. This analysis did not include some potentially significant socioeconomic and contextual variables such as average educational attainment, political stability, cultural practices, and urban-rural disparities in access to healthcare. It also relied on aggregated national-level data, which may mask regional or subpopulation differences within each country. Additionally, this study's retrospective and comparative nature does not allow for causal inferences, limiting the ability to establish direct relationships between economic development, health outcomes, and employment rates. Future research should incorporate more variables and use disaggregated data to better understand the determinants of life expectancy and economic outcomes in these countries.
CONCLUSION
This study investigated the relationship between socio-economic determinants of life expectancy in Nigeria, Algeria, and South Africa from 1991 to 2015. The variables examined included life expectancy, population growth, employment rates, GNI per capita, health expenditure, HIV prevalence, and infant and maternal mortality rates. The findings suggest that South Africa's BRICS membership provides significant economic resources and health partnerships that contribute to long-term development and improvements in life expectancy. However, Algeria's outcomes, which are comparable or even superior in some indicators despite not being part of BRICS, indicate that South Africa's affiliation is not a cure-all for socio-economic challenges. While BRICS membership offers clear advantages such as increased capital inflows and health support, South Africa's economic and health trends highlight the importance of domestic health policy, effective resource allocation, and targeted health interventions in transforming economic benefits into measurable improvements in life expectancy. Finally, building on this study, subsequent studies could employ mixed methods, incorporating qualitative interviews with policymakers, public health officials, and community leaders to contextualize the quantitative findings. Such an approach would provide a more holistic understanding of how international alliances like BRICS influence national strategies, illuminate institutional implementation challenges, and strengthen the evidence base for policy formulation across the continent.
AUTHORS' CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: G.I.: Data collection; O.S.S.: Data analysis or interpretation; O.K.: Visualization; S.B., Y.N.M., and E.Y.S.: Draft manuscript; All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| BRIC | = Brazil, Russia, India, China |
| GNI | = Gross National Income |
AVAILABILITY OF DATA AND MATERIAL
The data supporting the findings of the article is available within the article and in the bibliography.
ACKNOWLEDGEMENTS
Declared none.

