All published articles of this journal are available on ScienceDirect.

Evaluation of Knowledge Management Maturity at Shiraz University of Medical Sciences and Solutions for its Improvement: A Cross-Sectional Mixed-Methods Study
Abstract
Objective
This study aims to evaluate the Knowledge Management Maturity (KMM) and to provide solutions for its improvement at the Shiraz University of Medical Sciences (SUMS) in Iran.
Methods
This quantitative-qualitative cross-sectional study was conducted in 2022. Two hundred and ten experts in knowledge management completed the standard evaluation tool to assess knowledge management maturity. Semi-structured interviews were conducted with ten managers. Quantitative data were analyzed using descriptive statistics in Microsoft Excel 2013, while qualitative data were examined using framework analysis with MAXQDA 10.
Results
Knowledge management maturity was assessed at Level 3 (Expansion) with a score of 135.2. Technology scored the highest (21.6), while leadership scored the lowest (18.44). To enhance knowledge management, solutions were identified across the dimensions of leadership (collaborative management, culture building, implementation of motivational systems, executive regulations, and guidelines), people (training and empowerment of managers and staff, merit-based selection), technology (quantitative and qualitative development of IT infrastructure), and process (identification, creation, storage, sharing, and use of knowledge).
Conclusion
The solutions proposed in this study can be utilized to structure the stages of maturity, planning, and policymaking in knowledge management.
1. INTRODUCTION
Knowledge is vital for production, sustainable competitive advantage, and wealth generation, necessitating effective management [1]. Knowledge Management (KM) emerged as a response to the growing pressure on organizations to improve effectiveness and efficiency [2]. KM involves systematically creating, sharing, and applying knowledge to drive innovation and create value within organizations [3]. Health knowledge management also refers to the production, modeling, sharing, using, and translating knowledge to improve the quality of patient care and better manage health problems [4]. Effective KM contributes to improved social and economic outcomes and higher quality of care in healthcare organizations [5, 6].
Knowledge management maturity models, which describe the evolution of organizational KM over time, assess the maturity level, strengths, weaknesses, and areas for improvement [2, 7]. These models are essential tools for managers, as they facilitate the implementation of KM by guiding and overseeing programs, identifying barriers, and helping eliminate them [2, 8]. Several KM maturity models exist, including the American Productivity and Quality Center Knowledge Management Maturity Model (APQC KM), Siemens Knowledge Management Maturity Model, Intellectual Capital Management Capability Model, Social Network Scorecard for Assessing Knowledge Flow, Knowledge Generation Maturity Approach, People Capability Maturity Model, Knowledge Manager's Decision-making Guide, and the Asian Productivity Organization Knowledge Management (APO KM) [2, 8].
The APO KM tool helps organizations assess their knowledge management readiness across seven categories: leadership, process, people, technology, knowledge processes, learning and innovation, and KM outcomes. The results of this assessment provide a five-level readiness for KM within an organization, ranging from the lowest level of “reaction” to the highest level of “maturity” [8, 9]. According to the APO model, organizations differ in their level of KM maturity. Akay and Welly (2022) found an Indonesian financial and information technology company at level 4 (refinement) [10]. Similarly, Kurnia et al. (2021) assessed an Indonesian food and drug provincial office at level 4(refinement) [9]. Abu Naser et al. (2016) reported Palestinian universities at level 3 (expansion) [11], and Shafiee et al. (2022) in Iran found Kermanshah University of Medical Sciences at the same level 3 (expansion) [12].
At Shiraz University of Medical Sciences (SUMS), knowledge management was initiated in 2006 by the Office of Organizational Development and Administrative Transformation, initially focusing on the proposals committee. Efforts have included identifying, registering, evaluating, developing, and troubleshooting knowledge to motivate staff and promote engagement. Given the importance of assessing KM programs to identify strengths, weaknesses, and areas for improvement, and considering the absence of prior research on KM maturity at SUMS, this study was conducted in 2022 to evaluate KM maturity and propose strategies for its enhancement.
2. METHODS
This cross-sectional study employed a mixed-methods approach in 2022 at SUMS. The quantitative component assessed the knowledge management maturity level, while the qualitative component identified strategies for improving and developing it.
2.1. Quantitative Phase
The study population comprised 210 KM managers, experts, and representatives from university subunits-including faculties, hospitals, and health networks-selected via a census method. Knowledge management maturity was assessed using the APO KM tool. The questionnaire consisted of two sections: the first collected demographic data (gender, occupation, employment status, and education), while the second included 42 items across seven categories: KM leadership (1-6), process (7-12), people (13-18), technology (19-24), knowledge processes (25-30), learning and innovation (31-36), and KM outcomes (37-42). Items were rated on a five-point Likert scale from 'never' (1) to 'always' (5), with category scores ranging from 6 to 30 and a total score range of 42 to 210. Maturity levels were classified as reaction (42-83), initiation (84-125), expansion (126-146), refinement (147-188), and maturity (189-210) [8, 9]. Descriptive statistics (means and percentages) were used for data analysis, and results were visualized using Excel 2013.
2.2. Qualitative Phase
In the qualitative phase, 10 managers from SUMS were purposively selected to identify strategies for improving knowledge management. Inclusion criteria included a minimum of a bachelor's degree, over five years of managerial experience in healthcare, sufficient knowledge and expertise of KM, effective communication skills, and willingness to participate.
2.3. Data Collection
Data were collected using semi-structured interviews, which offered flexibility to explore participants' in-depth responses and enhance the validity of the findings [13]. The interviews began with three guiding questions: (1) What are the scientific and practical approaches to creating and developing knowledge management? (2) How can knowledge management be strengthened in the healthcare sector? (3) What role do managers play in designing and developing knowledge management?
2.4. Procedure
This study was approved by the Ethics Committee of SUMS (Code: IR.SUMS.NUMIMG.REC.1400.012). Informed consent was obtained from all participants before in-person interviews were conducted at their workplace when preferred and pre-arranged. The study objectives were explained at the outset, and we assured participants their information would remain confidential. Interviews, conducted by a research team member, lasted at least 60 minutes. With participants' permission, interviews were audio-recorded and transcribed verbatim shortly thereafter. Data collection continued until thematic saturation was reached.
2.5. Data Analysis
Framework analysis was used to analyze qualitative data, offering a transparent and structured approach commonly applied in health research. It allows researchers to create new theories from the data while focusing their analyses on predetermined research objectives. This method follows a structured sequence to systematically identify the themes in qualitative data [14, 15]. To ensure proper data interpretation and increase the study's accuracy and validity, we adhered to good practice guidelines in qualitative research [16, 17]. Therefore, a consensus approach was used to avoid relying on a single researcher's perspective. Two researchers analyzed the content and discussed and exchanged their opinions to reach an agreement in the case of disagreement.
Additionally, a respondent credibility checklist was used to confirm the data. The developed framework was sent to the participants for feedback to ensure their opinions were reflected [18]. Qualitative data were examined using framework analysis with MAXQDA 10.
3. RESULTS
Of the 210 distributed questionnaires, 184 were returned, yielding a response rate of 87.6%. Eleven participants declined to complete the questionnaire, and fifteen provided incomplete responses. The majority of respondents in the quantitative phase were male (53.3%), worked in healthcare (70.1%), held permanent positions (86.4%), and had a bachelor's degree (58.2%) (Table 1).
Assessment of knowledge management at SUMS using the APO KM tool revealed a maturity level of 3 (Expansion), with a total score of 135.2. The highest score was observed in the technology category (21.6), while the lowest was in knowledge management leadership (18.44) (Table 2).
The maturity level of knowledge management at SUMS is illustrated in a radar chart (Fig. 1), which presents the average score of each dimension relative to its maximum possible score. This visual representation highlights dimensions performing well and those requiring further development.
In the qualitative phase, most participants were male (70%), officially employed (80%), and held a master’s degree (50%). The mean age was 47.1 years, with an average of 22.2 years of work experience. Strategies for improving knowledge management were categorized into four main areas: leadership, people, technology, and process. Within the leadership domain, four subcategories emerged: collaborative management, culture building, implementation of a motivational system, and executive regulations and guidelines. The people category included training and empowerment of managers and staff and merit-based selection. In the technology category, participants emphasized quantitative and qualitative IT infrastructure development. The process domain encompassed five key subcategories: identification, creation, storage, sharing, and application of knowledge.
The findings also revealed the most frequent solution. The leadership category emphasized 'fostering a culture of brainstorming, teamwork, group formation, and idea generation'. In the people category, the most frequent solution was the 'proper use of databases for recording individuals' knowledge and making managerial decisions.' In the technology category, 'updating and developing computer hardware and software' was often highlighted. In the process category, the most frequent solution was 'providing employees with reports and feedback on knowledge management outcomes' (Table 3).
4. DISCUSSION
Knowledge is widely recognized as one of the most critical assets for gaining a competitive advantage in today’s organizational landscape and must be managed effectively [2]. Knowledge Management (KM) enhances team and organizational performance by strengthening intellectual capital and optimizing utilization [6]. According to the five-level maturity model developed by the Asian Productivity Organization (APO), KM maturity progresses through distinct stages. The first level, Reaction, is marked by a lack of awareness regarding KM and its role in enhancing productivity and competitiveness. At the second level, Imitation, organizations begin to recognize the importance of KM and initiate preliminary efforts. The third level, Expansion, reflects the broad adoption and implementation of KM practices across organizational units. The fourth level, Refinement and Control, systematically evaluates and continuously improves KM initiatives. At the highest level of Maturity, KM becomes a fully integrated and strategic function within the organization, occupying a dominant position in guiding decision-making and innovation [8, 12]. The assessment of Knowledge Management (KM) maturity at Shiraz University of Medical Sciences (SUMS) indicated that the institution is positioned at the third level-Expansion-of the APO KM maturity model. This level signifies that the university has initiated systematic knowledge-sharing practices within its core functions and has allocated resources specifically for KM activities. Similar findings have been reported in previous studies, where Kermanshah University of Medical Sciences (2022) and several Palestinian universities (2016) were also evaluated at the third level of maturity, reflecting an expanding phase of KM implementation [11, 12].
The highest knowledge management readiness score at SUMS was in the technology category, while the lowest was in leadership. The technology category evaluates the organization’s ability to implement knowledge-based solutions, like collaborative tools and content management systems, focusing on reliability and accessibility [8]. Similar studies showed the highest scores in technology at the Indonesian Food and Drug Administration and Kermanshah University of Medical Sciences [9, 12], aligning with this study’s findings. Knowledge management leadership assesses how well the organization addresses knowledge-based economic challenges through its policies, strategies, and leadership in sustaining knowledge practices [8]. A review study found that managers' knowledge management competencies included system management, professional development, and leadership behavior and attitude. However, there was a limited understanding of the competencies of healthcare managers in knowledge management [5].
The interviewees' proposed solutions for improving knowledge management were categorized into four areas: leadership, people, technology, and processes. Leadership was prioritized for policymaking and investment, as highlighted in the quantitative part of the study. Despite
|
Descriptive Statistics Demographic Characteristics |
N (%) | |
|---|---|---|
| Sex | Male | 98 (53.26) |
| Female | 86 (46.74) | |
| Occupational Field | Administrative & Financial | 38 (20.6) |
| Educational & cultural | 9 (4.9) | |
| Health & treatment | 129 (70.1) | |
| General | 4 (2.2) | |
| Information system | 2 (1.1) | |
| Technical & engineering | 2 (1.1) | |
| Type of employment | Permanent | 159 (86.4) |
| Temporary-to-permanent | 6 (3.3) | |
| Contractual | 19 (10.3) | |
| Educational level | Associate’s degree (A.S.) | 3 (1.6) |
| Bachelor’s degree (B.S.) | 107 (58.2) | |
| Master’s degree (M.S.) | 42 (22.8) | |
| Doctor of medicine (M.D.) | 23 (12.5) | |
| Doctorate (Ph.D.) | 9 (4.9) | |
| Categories | Score | Max Score | Ranking of Dimensions |
|---|---|---|---|
| KM Leadership | 18.44 | 30 | 7 |
| Process | 19.24 | 30 | 3 |
| People | 18.74 | 30 | 6 |
| Technology | 21.6 | 30 | 1 |
| Knowledge process | 19.03 | 30 | 4 |
| Learning & Innovation | 18.75 | 30 | 5 |
| KM outcomes | 19.4 | 30 | 2 |
| Sum | 135.2 | 210 |
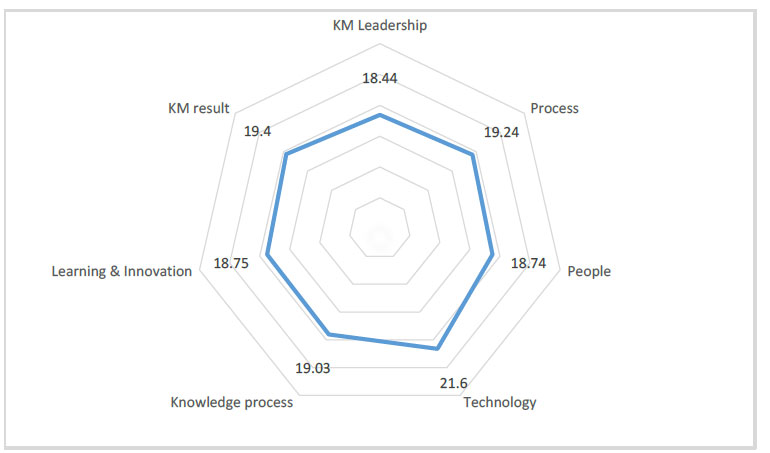
Radar Diagram of KM evaluation.
| Categories | Sub-categories | Codes | Frequency |
|---|---|---|---|
| Leadership | Collaborative management | Engaging employees across all hierarchical levels in meetings and decision-making committees | 10 |
| Setting clear, specific, measurable, and achievable knowledge-related objectives | 7 | ||
| Incorporating employee feedback into the development of the vision, mission, and goals of knowledge management | 4 | ||
| Identifying and addressing barriers to achieving organizational objectives through collaborative methods | 3 | ||
| Fostering trust and encouraging employee participation in knowledge sharing and reuse | 2 | ||
| Establishing a knowledge management committee with regular weekly meetings | 1 | ||
| Culture building | Promoting a culture of brainstorming, teamwork, collaboration, and idea-sharing | 16 | |
| Demonstrating strong commitment and support from senior management in developing knowledge management systems | 9 | ||
| Shifting the organization towards a learning-oriented, innovative, and knowledge-generating environment | 7 | ||
| Encouraging a culture of innovation and creativity | 7 | ||
| Transitioning organizational culture to one that is knowledge-driven | 5 | ||
| Establishing think tanks and promoting group ideation | 4 | ||
| Prioritizing and valuing knowledge and collaborative ideas | 4 | ||
| Creating a friendly and trust-based organizational climate | 4 | ||
| Fostering close communication between management and staff with attention to individual goals | 4 | ||
| Institutionalizing knowledge management practices within the organization | 2 | ||
| Implementation of a motivational system | Implementing appropriate incentive systems to encourage idea-sharing and knowledge transfer | 15 | |
| Offering tangible and intangible rewards aligned with employee needs and delivered promptly | 11 | ||
| Appreciating individuals and teams actively contributing to knowledge management | 7 | ||
| Engaging employees in the outcomes and benefits derived from effective knowledge management | 2 | ||
| Executive regulations and guidelines | Including knowledge management in employee and managerial performance evaluations | 5 | |
| Adopting a more interventionist and questioning approach to organizational development management in knowledge management | 4 | ||
| Embedding knowledge management considerations into all organizational plans and activities | 3 | ||
| Defining indicators to assess knowledge management performance across managers, employees, and units | 3 | ||
| Reducing bureaucratic procedures and excessive regulations | 2 | ||
| Stability of managers and organizational goals | 2 | ||
| Standardizing policies and procedures across all levels of the organization | 2 | ||
| Conducting continuous evaluations of knowledge management practices | 2 | ||
| Integrating knowledge management activities into employees’ job descriptions | 2 | ||
| People | Training and empowerment of managers and staff | Designing comprehensive and needs-based training programs focused on the job and knowledge-based management | 12 |
| Utilizing innovative training methods and diverse educational platforms | 8 | ||
| Disseminating knowledge management information via brochures and short messages | 6 | ||
| Assessing training effectiveness through various evaluation methods | 4 | ||
| Ensuring managers are aware of the strengths and weaknesses of the processes under their responsibility | 3 | ||
| Organizing visits to successful knowledge management centers | 2 | ||
| Conducting educational tours and seminars | 1 | ||
| Providing innovative-oriented training using scientific methods for motivated staff | 1 | ||
| Offering practical rather than solely theoretical instruction | 1 | ||
| Merit-based selection | Leveraging databases to capture individuals' knowledge and managerial decisions | 15 | |
| Emphasizing meritocracy by assessing competencies through recorded skills and qualifications | 10 | ||
| Recruiting competent, creative, and knowledgeable senior managers aligned with KM values | 9 | ||
| Hiring personnel based on skillsets aligned with organizational needs and fields of study | 8 | ||
| Recording and analyzing behavioral and professional assessment outcomes in databases | 3 | ||
| Technology | Quantitative IT infrastructure development | Updating and expanding organizational hardware and software infrastructure | 6 |
| Designing appropriate software related to employee databases | 1 | ||
| Qualitative IT Infrastructures Development |
Improving internet and intranet bandwidth and connectivity | 4 | |
| Enhancing the dissemination of KM outputs through digital platforms | 3 | ||
| Facilitating online delivery of KM information and training programs | 3 | ||
| Strengthening internal communication, information flow, and reciprocal learning | 2 | ||
| Process | Identification | Benchmarking against national and international knowledge management best practices | 6 |
| Using structured frameworks like the Building Blocks model as KM foundations | 1 | ||
| Implementing suggestion boxes to collect employee input | 1 | ||
| Compiling organizational issues for the KM committee to address | 1 | ||
| Creation | Supporting the development of raw ideas into executable proposals via the KM committee secretary mechanisms | 2 | |
| Applying structured problem-solving and lessons learned from prior experiences | 2 | ||
| Organizing on-site visits to address issues and generate immediate solutions | 1 | ||
| Storage | Preventing knowledge loss when employees leave the organization | 6 | |
| Establishing efficient mechanisms for knowledge documentation | 2 | ||
| Creating organizational knowledge maps and knowledge trees | 2 | ||
| Sharing | Communicating KM results to employees through structured reports | 9 | |
| Sharing the impact and effectiveness of each KM mechanism organization-wide | 3 | ||
| Disseminating KM outcomes to increase organizational awareness | 2 | ||
| Application of knowledge | Creating change within the organization through knowledge management | 4 | |
| Recognizing knowledge as a strategic organizational asset and capital | 1 |
two decades of experience in knowledge management at SUMS, progress has been made in process, technology management, and strategies for utilizing validated results. However, there is a clear need for policymaking and cultural development, particularly for university leaders who are key supporters of the knowledge management system. Effective healthcare leaders in knowledge management must exhibit coaching, role modeling, and active, exemplary behavior [5]. The study recommended strengthening leadership through collaborative management, cultural development, incentive systems, and clear regulations. The most frequently suggested solutions included promoting brainstorming sessions, teamwork, and using appropriate incentive systems to encourage knowledge sharing. Although there are various contextual challenges, including inadequate planning and strategies, weak organizational culture and structure, employee resistance to change, limited financial support, and a lack of awareness and capacity among employees to engage in knowledge management, these issues have also been identified as challenges in the implementation of knowledge management in other studies [19]. However, it seems that the solutions proposed by the interviewees could be somewhat effective in addressing these challenges. In a similar study conducted in Finland, health and social care managers identified that managerial competence in knowledge management is influenced by behavioral and attitudinal traits, interactive network competence, dimensions of knowledge management competence, knowledge management infrastructure, and organizational learning culture [20]. According to Ayatollahi and Zeraatkar's (2020) review, organizational culture had the greatest impact on knowledge management implementation in developed countries, while both organizational culture and information technology were most influential in developing countries within the healthcare sector [21]. Additionally, Khorbanizadeh et al.'s (2021) meta-analysis identified empowerment, participation, teamwork, and human resource management as the most critical factors for knowledge management success in Iran [22]. Other studies also emphasize the role of a collaborative culture in facilitating knowledge sharing [9, 23].
An organization’s capacity to promote employee learning and knowledge development is a key element of knowledge management within the people dimension. In healthcare, professional development and enhancing general and specialized competencies are essential for achieving excellence [24]. Participants in this study emphasized that training and empowering managers and employees, along with effective selection and management practices, should be central to the knowledge management strategy. Commonly suggested solutions include using databases to register individual knowledge and decisions and implementing face-to-face or workshop training programs on knowledge management benefits and methods. Competency, which involves applying knowledge effectively and creating economic and social value, is crucial in motivating individuals to share their knowledge [25]. Transparency in the appropriate selection and management of employees, facilitated by the creation of comprehensive databases, can effectively encourage individuals to share their knowledge.
Furthermore, health managers must prioritize the development of employees' professional skills in knowledge management through performance evaluations, training, organizational learning, and support for ongoing professional growth [5]. Innovative teaching methods are essential for fostering intellectual dynamism and innovation within knowledge management systems [10]. Evaluations of the Knowledge Management System in Canada’s mental health and addiction programs have emphasized the need to enhance training content and delivery. This finding is consistent with the results of the present study [3].
At Shiraz University of Medical Sciences (SUMS), knowledge management technology is viewed as a competitive advantage compared to other institutions, as emphasized in national and regional brainstorming sessions. However, experts have underscored the importance of developing quantitative and qualitative information technology infrastructures. Numerous studies have highlighted the pivotal role of information technology in the success of knowledge management [5, 21, 22]. Technological solutions, such as advanced search and retrieval capabilities, embedded content management workflows, and artificial intelligence for content identification and recommendation, have proven to be effective [3]. Therefore, it is crucial to continually develop and update the hardware and software of computer systems to align with emerging technologies.
Since 2006, SUMS has played a leading role in knowledge management, serving as the principal advisor to the Ministry of Health and Medical Education and as a model for other universities in Iran. The KM system at Shiraz University of Medical Sciences SUMS facilitates the implementation of five core KM processes: identification, creation, storage, sharing, and utilization. Targeted knowledge calls are developed and disseminated in response to challenges identified through brainstorming sessions, think tanks, and managerial site visits. Specialized training workshops, experience-sharing sessions, and peer-to-peer knowledge exchange among KM managers are regularly organized to support this framework. Key scientific and executive stakeholders are identified, and their tacit knowledge and expertise are systematically captured through interviews, case studies, and storytelling, enabling the reuse of their practical problem-solving approaches. Educational brochures and pamphlets are continuously distributed, and the implementation of transformative initiatives is actively encouraged. Selected registered ideas are designated as organizational challenges, with their resolution pursued through structured quality management, coordination, and follow-up mechanisms. Additionally, decision-making platforms are emphasized to facilitate the implementation of high-impact proposals that require significant infrastructure and cross-departmental collaboration. While employee knowledge sharing is a critical component of knowledge management, particularly in mitigating knowledge loss due to staff turnover, it is equally important for the organization to provide regular reports and feedback to employees regarding the outcomes of KM efforts [9].
Therefore, integrating a feedback mechanism into the organization's KM processes is essential. Previous research, including the study by Aryankhesal et al. (2020) conducted in Tehran's educational hospitals, has highlighted a significant and positive relationship between knowledge management and organizational health, underscoring the importance of knowledge-based strategies in healthcare institutions [26]. The proposed knowledge management model in Colombia's health system emphasizes flexibility, responsiveness to system needs, continuous learning and feedback, and integrating insights derived from external sources and internal teamwork. These characteristics are consistent with the approaches proposed in this study [27].
LIMITATIONS
The combination of quantitative and qualitative approaches was one of the strengths of this study. However, a limitation is the reliance on descriptive statistics due to the structure and size of the available data. Future research with larger and more comprehensive datasets is encouraged to apply advanced statistical techniques, such as regression, factor analysis, and time-series analysis, to gain deeper insights into the relationships among KM dimensions. Additionally, since this study was conducted at SUMS as a single organization, its results may not be generalizable to other organizations. The proposed solutions for this organization and other medical universities will likely have more practical applications. Another limitation is the absence of a dedicated group to implement the proposed solutions. Future research should consider including such a group to better evaluate their effectiveness.
CONCLUSION
Creating an appropriate platform for utilizing knowledge to achieve the vital mission of the health system is essential.Equally important is understanding the organization’s current status in knowledge management and identifying factors that influence decision-making to effectively employ and improve KM. SUMS was assessed at Level 3, the development stage of knowledge management. The highest and lowest readiness scores were in the categories of technology and knowledge management leadership, respectively. Maintaining strengths and addressing weaknesses based on the proposed solutions in this study can help prioritize efforts in organizing maturity stages, planning, and policymaking in knowledge management at SUMS, thereby providing a foundation for organizational interventions.
AUTHORS' CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: N.A.N: Study conception and design; M.H.R: Data collection; N.B. Writing - original draft preparation;. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| KMM | = Knowledge Management Maturity |
| SUMS | = Shiraz University of Medical Sciences |
| APO | = Asian Productivity Organization |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the ethics code of IR.SUMS.NUMIMG.REC.1400.012 at SUMS, Iran.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
After obtaining informed consent, we interviewed in person, preferably at the participants' workplace, based on their preferences and previous coordination with them.
AVAILABILITY OF DATA AND MATERIALS
The data supporting this study's findings are available from the corresponding author [N.B] upon reasonable request.
ACKNOWLEDGEMENTS
The authors thank Shiraz University of Medical Sciences, Shiraz, Iran, the Center for Development of Clinical Research of Nemazee Hospital, and Dr. Nasrin Shokrpour for their editorial assistance.

