All published articles of this journal are available on ScienceDirect.

Dynamic Overview of Brucellosis Outbreaks in Humans and Animals in Bulgaria and the European Union
Authors Info & Affiliations
Abstract
Introduction/Objective
Brucellosis is a zoonotic disease with substantial public health and economic impact, requiring coordinated surveillance across human and animal populations. Bulgaria has historically been considered free of bovine brucellosis; however, re-emergence has been observed in recent years. The objective of this study was to analyze long-term epidemiological trends of brucellosis in humans and animals in Bulgaria (2002–2024).
Methods
Official surveillance data on laboratory-confirmed human cases and registered animal outbreaks were obtained from national and international databases. Descriptive statistics and linear regression analyses were performed using SPSS. Annual human cases were modeled against logarithmically transformed animal outbreak counts.
Results
Globally, animal brucellosis outbreaks increased in most regions, with the largest rises in the Americas (46%) and Asia (10%), while Europe showed a 46% decrease. The largest number of human cases in the EU/EEA was reported in 4 countries, with sporadic cases in 10 other countries. In Bulgaria, re-emergence was concentrated in border districts. A statistically significant association was observed between annual animal outbreaks and human cases during 2006–2023 (R2=0.488; p=0.043). When 2024 data were included, the association was attenuated (R2=0.214; p=0.18).
Discussion
The extensive integrated analysis of human brucellosis cases and registered animal outbreaks over the past decade supports updated mapping of human brucellosis worldwide, taking into account a complex of sanitary, socio-economic, and political conditions.
Conclusion
The findings on the emergence and re-emergence of brucellosis indicate renewed transmission risks and highlight gaps in prevention and surveillance systems despite advances in diagnostics.
1. INTRODUCTION
Among the factors involved in the transmission of infections to humans, domestic animals play a key role, as many pathogens may increase their pathogenicity within animal hosts. Along with increased direct contact between animals and humans in daily activities, these interactions raise the risk of contracting many zoonotic diseases, which is one of the reasons that led in 2013 to action by 32 World Health Organization (WHO) Member States to address 17 neglected zoonoses, including brucellosis [1]. Brucellosis is caused by Gram-negative aerobic bacteria belonging to the genus Brucella. The disease has an incubation period ranging from 5 to 60 days [2]. It was described in humans two millennia ago [3] and was first isolated from the spleen of a soldier who died from the infection in 1884 [4].
Brucellosis remains one of the most widespread bacterial zoonoses worldwide, with persistent transmission in parts of the Mediterranean basin, the Middle East, Central and South Asia, sub-Saharan Africa, and Latin America. Recent global modeling estimates suggest that more than 500,000 new human cases occur annually; however, the true burden is likely substantially higher due to underdiagnosis, limited laboratory capacity, and incomplete surveillance reporting in endemic regions [5, 6]. In addition to its impact on human health, brucellosis continues to impose significant economic losses in the livestock sector through reproductive failure, decreased productivity, trade limitations, and the financial costs associated with long-term eradication programs [7, 8].
Human infection occurs primarily through exposure to infected livestock or through consumption of unpasteurized dairy products [5]. The disease often presents with non-specific clinical manifestations such as prolonged fever, fatigue, night sweats, and musculoskeletal pain, frequently resulting in delayed diagnosis and chronic complications [9]. Among the species pathogenic to humans, Brucella melitensis is most commonly associated with severe disease and outbreak situations, particularly in regions where small ruminant infection remains insufficiently controlled [10].
The epidemiology of brucellosis is closely linked to the effectiveness of veterinary control measures. Countries that have achieved official disease-free status in livestock have substantially reduced human incidence; however, sporadic outbreaks and re-emergence events continue to occur, especially in border regions adjacent to endemic areas. Increased cross-border animal movement, informal trade, and population mobility create ongoing vulnerabilities despite harmonized surveillance frameworks within the European Union. These challenges highlight the importance of integrated One Health approaches that combine veterinary and public health surveillance systems to prevent re-establishment of transmission in historically free countries [11, 12].
Although autochthonous brucellosis in cattle and small ruminants existed in the past, Bulgaria has been considered free from this infection since 1958 [13]. Over the subsequent 50 years, rare epizootics were recorded due to the importation of infected animals [14, 15]. Until 1980, infected cattle were imported into Bulgaria several times from Central and Western European countries [15, 16]. During one of these B. abortus outbreaks, 32 livestock breeders and veterinary specialists were infected and diagnosed at the National Diagnostic Research Veterinary Medical Institute.
Nowadays, brucellosis has re-emerged as an infection in Bulgaria. A number of political and socio-economic changes in the country are a prerequisite for this. The principle of free circulation of goods and individuals within the European Union is a fundamental policy of the Community, but it also has some negative effects, such as the appearance of the aforementioned disease in humans and animals in our country. During the period 2005–2015, one outbreak of epidemic-related imported cases (2005) and two autochthonous outbreaks were registered, occurring in 2006–2008 and 2015 [15, 17, 18].
The annual number of new human brucellosis cases remains uncertain [19], despite the significant social and economic impact of the disease. For decades, attempts have been made to identify the global and regional impact of this disease, as well as to establish, through documented evidence, the annual number of new cases. However, the global incidence of the disease cannot be accurately determined due to the fact that the annual incidence cannot be estimated solely from human cases of brucellosis reported to intergovernmental public health institutions because of incomplete data records and a lack of representation between geographical regions [6].
In the present paper, in order to increase the knowledge of all stakeholders – scientists, human and veterinary doctors, laboratory specialists, and public health experts- a follow-up analysis of reported cases in humans and animals was carried out.
2. MATERIALS AND METHODS
The study analyzed the current national regulations regarding brucellosis and the measures taken to detect it in humans and animals by the Ministry of Health and the Ministry of Agriculture and Food, through the relevant national disease control and surveillance authorities. For the purpose of the study, the incidence of registered cases of brucellosis in humans and animals for the period 2002 – 2024 was analyzed. Official data on brucellosis outbreaks in animals from Bulgarian Food Safety Agency (BFSA) reports and data on human cases processed for reporting and control purposes by the National Center for Public Health and Analyses (NCPHA), as well as laboratory data from the National Reference Laboratory “Especially Dangerous Bacterial Infections” (NRL EDBI) at the National Center of Infectious and Parasitic Diseases (NCIPD), were systematically reviewed and analyzed for the study period. The differentiation of the Brucella species was performed through real-time PCR, and the detected strains were further subtyped by Multiple-Locus Variable number tandem repeat Analysis based on 16 loci (MLVA16).
To prevent double-counting of human cases, records from NCPHA and NRL EDBI were cross-validated using case identifiers (initials, age, district, and year of reporting). NRL EDBI serves as the national confirmatory laboratory; therefore, discrepancies were resolved in favor of laboratory-confirmed data. No duplicate cases remained after reconciliation.
This study included only officially reported and laboratory-confirmed cases of human brucellosis and registered animal outbreaks that were notified to national, European, and international surveillance systems. For the analysis of Brucellosis cases in humans, the following inclusion criteria were applied: all laboratory-confirmed cases of Brucellosis reported to the National Center for Public Health and Analyses (NCPHA) during the study period; cases confirmed by the National Reference Laboratory for Especially Dangerous Bacterial Infections (NRL EDBI) based on microbiological culture and/or serological testing in accordance with national diagnostic guidelines; cases classified as “confirmed” or “probable” according to Ordinance No. 21 of July 18, 2005 on the registration, notification and reporting of communicable diseases; cases with complete information on year of diagnosis and district of residence. Suspected cases without laboratory confirmation or cases lacking essential epidemiological data (year or district) were excluded from the analysis.
The requirements for inclusion of animal outbreaks in the analysis were: all officially declared Brucellosis outbreaks in domestic livestock (large and small ruminants) reported by the Bulgarian Food Safety Agency (BFSA); outbreaks confirmed through serological and/or bacteriological testing in accordance with national veterinary regulations; outbreaks formally registered under the National Program for Prevention, Surveillance, Control and Eradication of Animal Diseases and Zoonoses. Excluded from the study were: suspected but non-confirmed outbreaks; reports lacking laboratory confirmation; and wildlife cases not included in official livestock surveillance records.
At the time of the study, no formally established or legally regulated framework existed in Bulgaria for routine joint epidemiological investigations conducted by both public health and veterinary authorities following confirmed brucellosis cases. The integrated analysis presented in this study was conducted collaboratively by the authors, who are recognized specialists representing the relevant national institutions responsible for human and animal brucellosis surveillance.
For epidemiological information at the European and global levels, data on disease outbreaks in domesticated animals were derived from public reports by the European Food Safety Authority (EFSA) and the World Animal Health Information System (WAHIS).
Data on human brucellosis cases within the EU were obtained and analyzed using surveillance reports published by the European Centre for Disease Prevention and Control (ECDC).
Additional data were obtained from international organizations responsible for the global surveillance, control, and management of zoonoses, including brucellosis, through their official websites.
The diagnosis of brucellosis is complex and is based on microbiological examination, supported by clinical presentation and epidemiological investigation of the circumstances leading to infection. Laboratory confirmation of brucellosis in humans includes bacteriological examination of blood for blood culture (at the beginning of the disease and during febrile attacks), bone marrow, and other materials according to the localization of the disease. Serological examination of blood is performed at all stages of the disease. Clinical materials are collected, packaged, and transported in compliance with the conditions for working with NRL EDBI according to the Instructions for taking materials for microbiological examination for brucellosis, described in the Information Journal 4/2007 of NCIPD and available on the Center's website. Properly packaged clinical material is sent to NRL EDBI at the NCIPD together with a covering letter and a duly completed questionnaire supporting the interpretation of the laboratory results and the epidemiological study. The examination is performed in the manner specified in the Methodological Instructions of the Ministry of Health No. 2 of 19.01.2004 for microbiological diagnosis of brucellosis.
Ethical approval was not required for the purpose of the investigation. This study was based on a retrospective analysis of secondary, fully anonymized surveillance data. According to national regulations, ethical review and approval were not required because no identifiable human or animal data were used.
The combined data on registered brucellosis outbreaks in animals and reported human cases were processed using statistical software (IBM SPSS Statistics for Windows, Version 26.0; IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize annual frequencies and rates of human cases and animal outbreaks. Trends across continents were compared using paired t-tests based on annual outbreak counts (2010–2022). To evaluate the association between animal outbreaks and human cases in Bulgaria, linear regression analysis was performed. The dependent variable was the annual number of laboratory-confirmed human cases. The independent variable was the annual number of registered animal outbreaks. Due to right-skewed distribution and the presence of extreme values, animal outbreak counts were logarithmically transformed using log10(x+1). Years with zero outbreaks were retained through this transformation.
Two regression models were constructed: a national annual model (2006–2023) and a district-level aggregated model (district–year observations). A sensitivity analysis including 2024 data was performed to assess the influence of high-leverage observations.
Statistical significance was defined as p < 0.05. No correction for multiple comparisons was applied because analyses were hypothesis-driven and limited in number.
3. RESULTS AND DISCUSSIONS
According to the provisions of Ordinance No. 21 of July 18, 2005, on the registration, notification, and reporting of communicable diseases, all cases of brucellosis in humans in the Republic of Bulgaria are registered and reported in accordance with the following classification: probable case of a communicable disease and confirmed case of a communicable disease.
The registration of the disease is carried out by medical institutions, health offices in schools, childcare facilities, specialized institutions for the provision of social services, and by regional health inspectorates.
Registration in the laboratory journal and reporting to regional health inspectorates of positive results for the disease are carried out by all medical-diagnostic laboratories, independent or within the structure of another medical or health institution.
The National Reference Laboratory, Section “Bacteriology and Bacterial Diseases” at the National Diagnostic Research Veterinary Institute in Sofia performs serological testing of samples from Large Ruminants (LRV) and Small Ruminants (SRV) and sends the results to the Bulgarian Food Safety Agency and the relevant Regional Food Safety Directorates (RFSD) for declaration of an outbreak in livestock facilities in accordance with Regulation No. 23 of 14.12.2005 on the procedure and manner for declaration and registration of contagious animal diseases, which determines the procedure and conditions for declaration of contagious diseases, as well as the notification of animals that have reacted positively.
The Bulgarian Food Safety Agency (BFSA) under the Ministry of Agriculture and Food is a central competent authority within the meaning of Art. 4 of Regulation (EU) 2017/625 of the European Parliament and of the Council of 15 March 2017 on official controls and other official activities performed to ensure the application of food and feed law, rules on animal health and welfare, plant health and plant protection products. BFSA interacts with institutions that participate in the Brucellosis in Large Ruminants Surveillance Program, respectively, the Brucellosis (Brucella melitensis) Surveillance Program in sheep and goats in Bulgaria, which has a duration of three years. Before the end of the three-year period of implementation of the above-mentioned programs, they are updated in accordance with the epizootic situation in the country under the terms of the Law on Veterinary Medical Activity. Both Brucellosis programs are part of the National Program for Prevention, Surveillance, Control, and Eradication of Animal Diseases and Zoonoses, which is implemented and controlled by the competent authority - the Bulgarian Food Safety Agency.
After brucellosis outbreaks were detected and declared, the BFSA implemented measures in accordance with the provisions of the national Ordinance No. 52 of 28 April 2006 on the health requirements for sheep and goats when moving or transporting them between the Republic of Bulgaria and the Member States of the European Union, to determine the health status of the establishments from which they originate and the additional guarantees for the health status of these establishments to prevent the free movement of live animals from the affected areas, control the spread of the disease, collect information and prepare reports with the results of the programs to the European Commission on the activities conducted in relation to the disease.
3.1. Surveillance and Monitoring of Brucellosis in Animals
In accordance with the procedure laid down in Commission Implementing Regulation (EU) 2020/2002 of 7 December 2020 laying down rules for the application of Regulation (EU) 2016/429 of the European Parliament and of the Council with regard to Union notification and Union reporting of listed diseases, at the EU level, brucellosis is reported through the Animal Disease Information System (ADIS).
The epizootic situation of brucellosis in the Republic of Bulgaria, the EU, and globally is illustrated in Figs. (1 and 2) and Table 1, summarizing outbreaks reported by individual countries during the period 2002–2024.
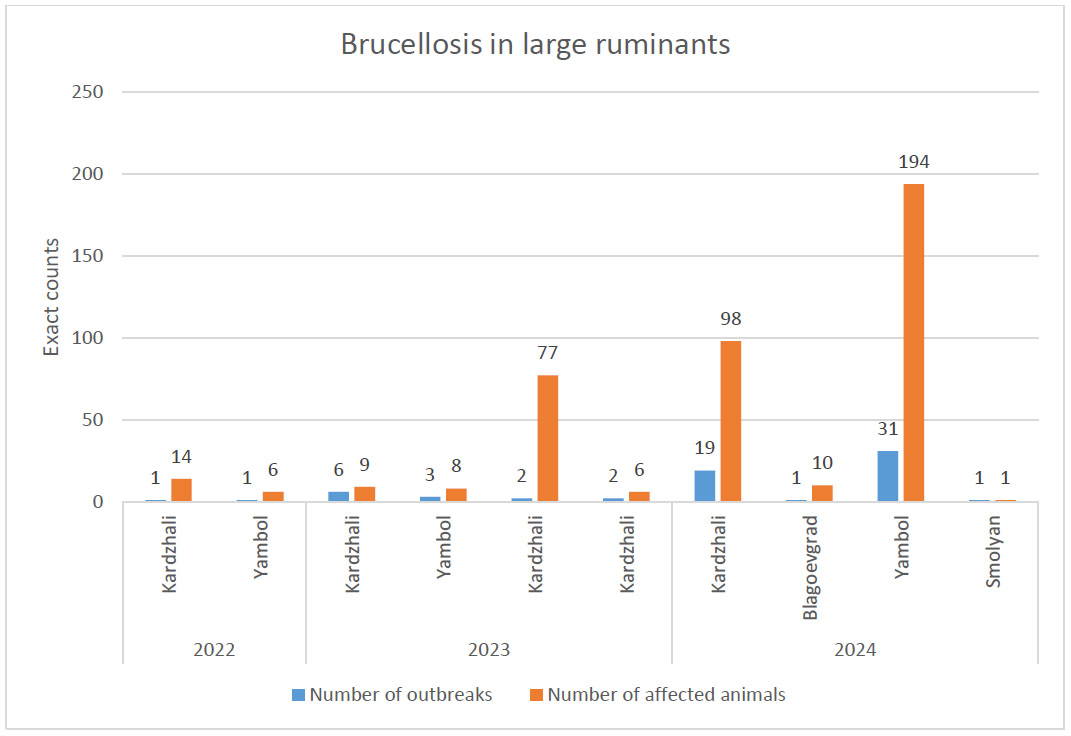
p>Dynamics of Brucellosis outbreaks in large ruminants in the Republic of Bulgaria, 2002-2024.
Source: Decisions of the Council of Ministers of the Republic of Bulgaria1
Data on the number of affected animals includes the number of animals destroyed.
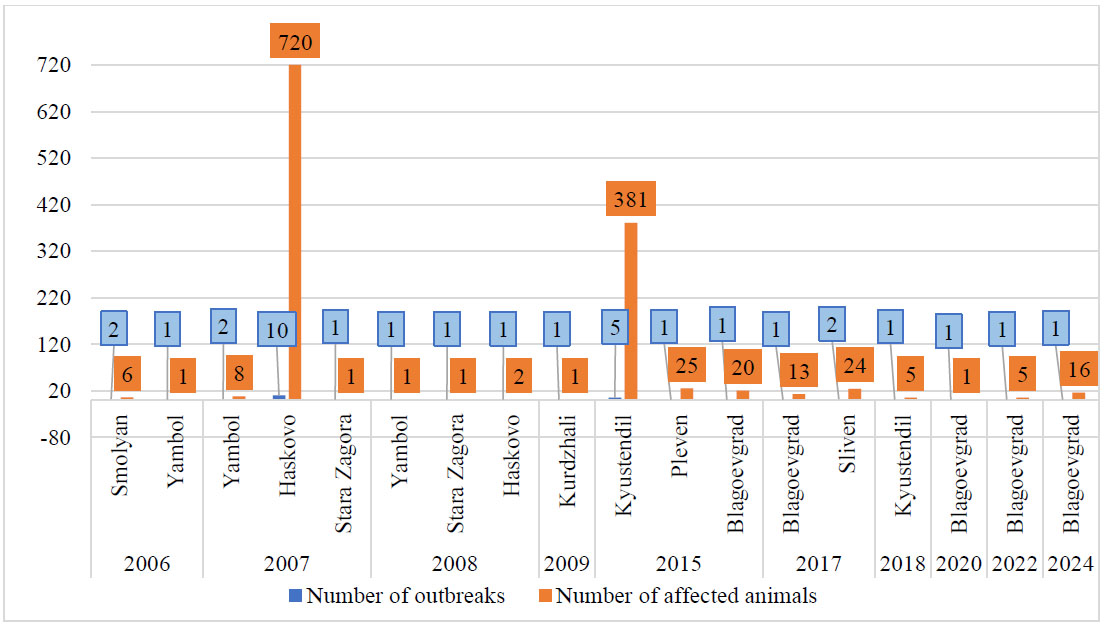
Dynamics of Brucella melitensis outbreaks in small ruminants in the Republic of Bulgaria, 2002-2024.
Source: Decisions of the Council of Ministers of the Republic of Bulgaria.
*Data on the number of affected animals includes the number of animals destroyed.
| World Region | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 |
Percentage Change 2010/2022 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Africa | 265 | 258 | 252 | 287 | 291 | 387 | 341 | 332 | 382 | 382 | 271 | 249 | 266 | 0% |
| Americas (North and South) | 529 | 515 | 548 | 633 | 634 | 838 | 901 | 984 | 967 | 921 | 744 | 790 | 772 | ↑ 46% |
| Asia | 918 | 1131 | 1082 | 1052 | 841 | 1002 | 1036 | 1209 | 1264 | 1325 | 1038 | 980 | 1012 | ↑ 10% |
| Europe | 587 | 600 | 498 | 509 | 536 | 586 | 524 | 624 | 428 | 368 | 387 | 328 | 318 | ↓ 46% |
Source: World Animal Health Information System (WAHIS)2.
Autochthonous brucellosis in large ruminants in the Republic of Bulgaria until 2022 has not been registered since 1958, when the last outbreak of the disease in cattle was detected. Figure 1 shows that in 2022, the first two outbreaks for the country occurred in Yambol district in November and Kardzhali district in December – both administrative regions having borders with neighboring countries (Yambol with Turkey, Kardzhali with Greece). In the reported outbreak in Yambol district, 6 animals were affected and destroyed, and in Kardzhali, the number of destroyed animals was 14. In 2023, the number of outbreaks detected increased, with the affected regions in the country remaining once again the border districts of Kardzhali and Yambol. The outbreaks in Kardzhali district were conditionally divided into three groups (Fig. 1), as they were detected in different months of the year. The first 6 were detected in the period from January to October in four livestock farms, with the number of animals affected being 9. A second outbreak of brucellosis in Kardzhali district was detected in November, when, in addition to Kirkovo municipality, where the first 6 outbreaks for 2023 were detected, the disease was also detected in Kardzhali municipality. During the third outbreak of the disease in Kardzhali district in December, a smaller number of animals were infected - 6, compared to November, when there were 77.
In 2024, the number of affected animals increased significantly, and in addition to the districts of Kardzhali and Yambol, which reported outbreaks in previous years, the disease spread and was reported from two more border districts - Blagoevgrad district (bordering Greece and the Republic of North Macedonia), where one outbreak with 10 affected large ruminants was reported, and Smolyan district (bordering Greece) with a sporadic outbreak and one affected animal.
In the Yambol district, the highest number of outbreaks (31) was reported, with the largest number of affected animals (194), while in the Kardzhali district, 19 outbreaks were reported and 99 animals were destroyed.
In June 2006, the first epizootic outbreaks in sheep and goats were identified in the Smolyan region. By the end of 2008, the disease had been registered in 18 settlements in 4 regions – Smolyan (bordering Greece), Yambol (bordering Turkey), Haskovo (bordering Turkey), and Stara Zagora, where the peak was recorded in the Haskovo district with 10 outbreaks of Brucella melitensis (Fig. 2).
As in the previous epizootic, during the period 2005 - 2008, the infection of goats was significantly higher than that observed in sheep, as it ranged from 2 to 87% for individual herds in goats and from 1 to 22% in sheep.
1Decisions of the Council of Ministers of the Republic of Bulgaria. (2016, 2019, 2022). Website https://www.strategy.bg/ bg/pris [accessed 18 March 2025]
2World Animal Health Information System (WAHIS). brucellosis outbreaks 2019-2022. Website https://wahis.woah.org/#/ dashboards/qd-dashboard [accessed 18 March 2025]
In 2015, compared to the period 2009 – 2014, the number of outbreaks increased significantly, as in 2015, 5 outbreaks with 381 affected animals were found in Kyustendil district (bordering Serbia and the Republic of North Macedonia). In fact, B. melitensis is confirmed to be endemic in North Macedonia, although there is a vaccination program for small ruminants has been ongoing since 2008 [20]. During the indicated period, there was one sporadic outbreak reported in Kardzhali district, in which 1 head of cattle was destroyed. In this epizootic, the infection rate in goats ranged from 2.1% to 57%, and in sheep, from 4.2%.
The total number of reported outbreaks in the period 2016 - 2022 was 6, with 3 of them in 2017 in the districts of Blagoevgrad (1 outbreak) and Sliven (2 outbreaks), with a total number of affected animals of 13 and 24, respectively. In 2018, 2020, and 2022, one outbreak for each year was reported in the districts of Kyustendil and Blagoevgrad, which shows a lasting trend of decreasing the occurrence of the disease in the country.
Considering that brucellosis outbreaks were predominantly detected in Bulgarian regions bordering neighboring Balkan countries, the transboundary nature of the threat is further confirmed as epidemiological reports since 2002 give evidence on outbreaks caused by B. melitensis in North Macedonia, Serbia, and Greece, and B. abortus in Greece [21].
Examining international trends in brucellosis, data presented in Table 1 indicated that, during the study period, the highest number of brucellosis outbreaks in domestic animals was reported in Asia, followed by a comparable number in the Americas, while Africa and Europe recorded lower overall numbers of outbreaks over the years.
Name of the disease according to WAHIS: Brucella abortus (Inf. With), Brucella melitensis (Inf. with), Brucella suis (Inf. with), Ovine epididymitis (Brucella ovis).
It is important to highlight that a relative change was observed over the investigated years across regions. In one region, there was no change in the occurrence of reported outbreaks (Africa (0%)), in two regions it increased, with a higher proportion observed in the Americas (46%) than in Asia (10%), and the only region where a decrease was observed was Europe, with a decline of 46% over the studied period.
Moreover, brucellosis outbreaks recorded for Europe in WAHIS are reported by more countries within the European continent than the number of the 27 EU member states and the United Kingdom (Northern Ireland) that provide data for the annual reports of EFSA and ECDC.
3.2. Surveillance and Monitoring of Brucellosis in Humans
Results from registered cases of people suffering from brucellosis in Bulgaria for the period 2002 - 2024 are presented in Fig. (3).
For the registered cases of the disease during the years indicated in Fig. (3), it is necessary to note that no deaths related to brucellosis were reported during the study period.
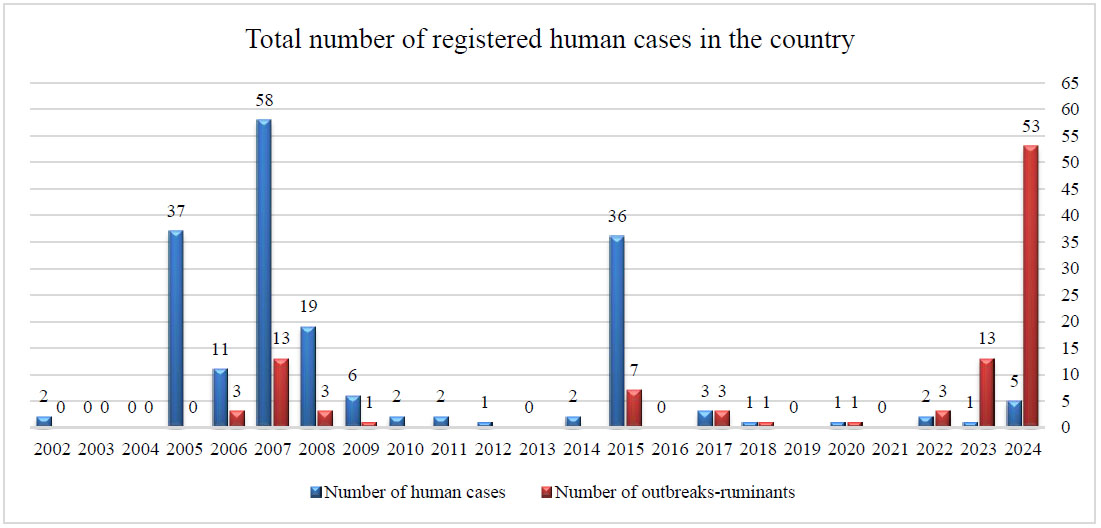
Distribution of reported cases of brucellosis in patients in Bulgaria by year, 2002 – 2024.
Source: National reference laboratory “especially dangerous bacterial infections”, national center of infectious and parasitic diseases.
It is also clearly seen that in six calendar years there were no registered infected people, namely in 2003, 2004, 2013, 2016, 2019, and 2021. The number of people diagnosed with brucellosis for the entire period is relatively small compared to the entire population of the country, which, according to data from the National Statistical Institute for 2002, was 7,845,841 people, and as of August 1, 2024, was 6,699,789 people. In general, it can be stated that registered cases of people infected with Brucella spp. were sporadic, with the exception of five calendar years - 2005, 2006, 2007, 2008, and 2015, where 37, 11, 58, 19, and 36 people diagnosed with brucellosis were identified, respectively
Despite the relatively small number of cases in humans and taking into account that Bulgaria is not an endemic region for the disease, one should not underestimate the fact that brucellosis is a newly emerging, particularly dangerous zoonosis in the country, in which all cases in humans are directly related to contact with infected animals and/or consumption of contaminated food [22]. Regression analysis demonstrated a statistically significant association between human cases and animal outbreaks registered during 2006–2023 (R2=0.488, p = 0.043) showing that about 48.8% of the variation in the number of human cases is explained by the logarithmically transformed value of outbreaks in animals (due to the presence of an extreme value in 2024, 53 animal outbreaks and 5 human cases, which substantially affected the linear relationship and the residual distribution, this case was excluded from the analysis).
Figure 4 presents data on the number of people infected and the areas in which they were diagnosed in the period 2002 – 2024. The results indicated that four peaks of the disease stood out, which were in different years of the studied period and with varying values, but mainly in several recurring areas where infected animals were registered as well (Haskovo, Kyustendil, Yambol, Kardzhali – all of them bordering regions).
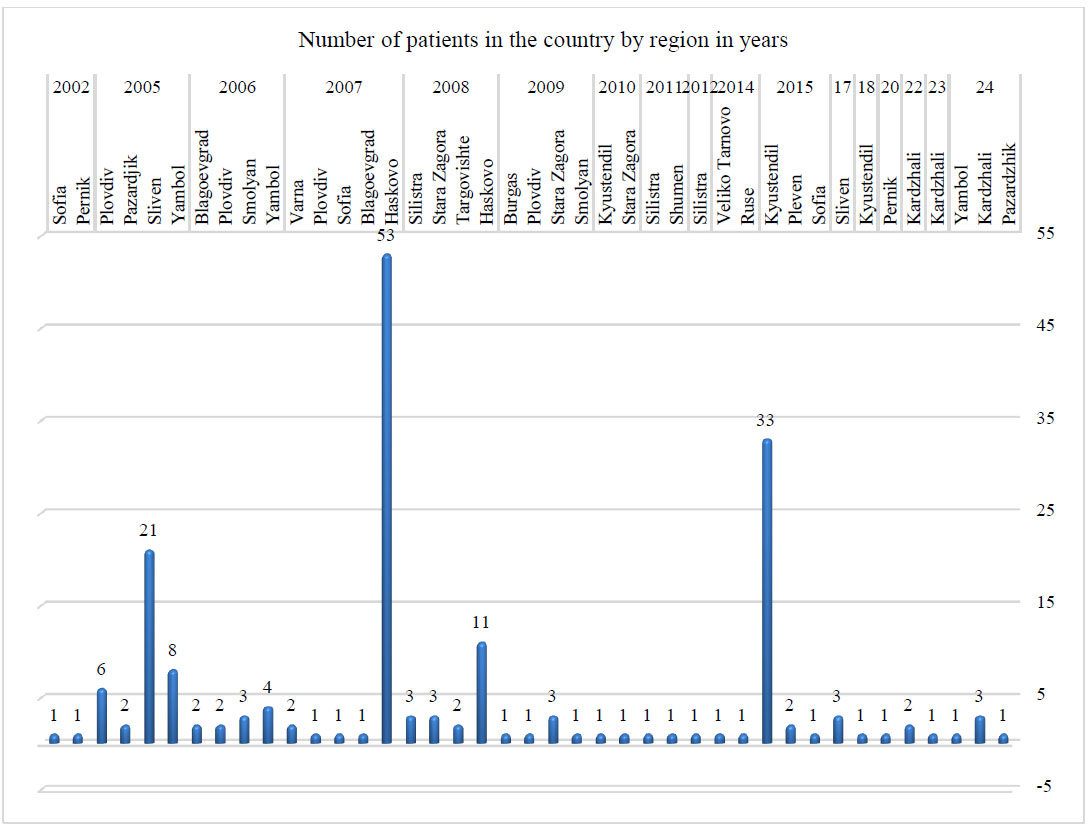
Registered cases of brucellosis in patients in Bulgaria by area in the period 2002 – 2024.
Source: National reference laboratory “especially dangerous bacterial infections”, national center of infectious and parasitic diseases.
According to BFSA data, brucellosis caused by Brucella melitensis has been eradicated in Bulgaria since 1941 [17]. The infection reappeared in 2005, when new imported cases were identified in the Sliven district in 37 people who worked on livestock farms in Northern Greece. In the following year, 2006, 11 cases were identified in humans, forming the first autochthonous outbreak in the country for more than 50 years. The most severe epidemic situation was in Haskovo district, where infected people were registered in two consecutive years - in 2007 with 53 and in 2008 with 11 people.
The last peak of the disease, coinciding with the second autochthonous outbreak, occurred in 2015, with a total of 36 epidemiologically related cases, of which 33 were in Kyustendil district, 2 in Pleven district, and 1 in Sofia city. It is important to highlight that even after the diagnoses of the first people infected with brucellosis were confirmed by the NRL EDBI, the Regional Food Safety Directorate (RFSD) was informed about the epidemic situation that had arisen. As a result, outbreaks of brucellosis in animals in the Kyustendil and Pleven districts were also detected in a timely manner. It is worth noting that when control measures were implemented by the veterinary authorities, the disease was not detected in any susceptible pigs. The positive effect of the timely interaction between human and veterinary medical specialists and the relevant responsible authorities is unquestionably demonstrated by a decrease in the number of sick people in the following years. The total number of cases in 2024 decreased to 12, of which 4 were reported in the latter part of 2024 (Fig. 4). These data do not show clear trends in incidence, as after a long period of absence of the disease in the country, it reappears and causes infection of different numbers of people and different types of animals in different areas. Regarding the molecular typing of the bacteria in confirmed human cases, through a standardized real-time PCR method, the Bulgarian isolates were identified as Brucella mellitensis, with their strains assigned to the Eastern Mediterranean genetic group.
Regression analysis demonstrated a statistically significant association between annual human cases and logarithmically transformed animal outbreaks during 2006–2023 (R2=0.488; p=0.043), indicating that approximately 48.8% of the variation in human cases was explained by outbreak frequency in animals. When 2024 data (53 animal outbreaks; 5 human cases) were included, the association was attenuated (R2=0.214; p=0.18). Diagnostic analysis showed that the 2024 observation exerted high leverage (Cook’s distance >1) and influenced residual distribution; therefore, results are presented both with and without this value.
However, statistically a significant dependence was found between the number of outbreaks in animals and human cases in the same residential area after aggregating the results at the district level and applying regression analysis (R2=0.205; p = 0.039), meaning that for every logarithmic increase in the number of outbreaks, the number of human cases is expected to increase. Geographic location alone did not significantly predict human case counts (p=0.34).
3European Centre for Disease Prevention and Control (2013-2022). Annual epidemiological reports. Brucellosis. Stockholm: ECDC [online]. https://www.ecdc.europa.eu/en/ publications-data/monitoring/all-annual-epidemiological-reports [accessed 20 March 2025]
Brucellosis is one of the most widely reported zoonoses, documented in more than 170 countries worldwide; however, it remains a frequently neglected disease. Contacts between animals and humans in the context of international trade and travel contribute to the continuous threat of emerging and re-emerging infectious diseases. Therefore, surveillance, mandatory consumption of pasteurized milk, the introduction of a reporting obligation by all countries in the world, strict restrictions on animal movements, and health education are important for managing the emergence and spread of the disease, as in most countries the disease is characterized by a period of several years with a low incidence rate, followed by an increase in the number of registered cases. This phenomenon is observed in southern and central Europe, including Greece, Albania, the Republic of North Macedonia, Bosnia and Herzegovina, Italy, Spain, and Portugal. Sporadic and imported cases are observed in countries in Western Europe, such as France, Germany, and the United Kingdom [19].
Table 2 presents data on the prevalence of brucellosis among EU member states, including Bulgaria, tracking the reported cases from the respective countries where brucellosis was diagnosed in humans in the period 2010 - 2022. Data were collected from the ECDC annual reports extracted from TESSy from EU/EEA countries for the period 2010-2022, with the corresponding numbers and rates of brucellosis cases per 100,000 population.
| Country | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RC | RC | RC | RC | RC | RC | RC | RC | RC | RC | RC | RC | RC | ||||||||||||||
| N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | N | R | |
| Austria | 3 | 0 | 5 | 0.1 | 2 | 0 | 7 | 0.1 | 1 | 0 | 1 | 0.01 | 4 | 0.05 | 6 | 0.07 | 7 | 0.08 | 6 | 0.07 | 8 | 0.09 | 6 | 0.07 | 7 | 0.08 |
| Belgium | 0 | 0 | 5 | 0 | 4 | 0 | 0 | 0 | 1 | 0 | 9 | 0.08 | 4 | 0.04 | 8 | 0.07 | 9 | 0.08 | 3 | 0.03 | 4 | 0.03 | 7 | 0.06 | 3 | 0.03 |
| Bulgaria | 2 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 2 | 0 | 36 | 0.5 | 0 | 0 | 2 | 0.03 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 0 | 0 | 2 | 0.03 |
| Croatia | * | * | * | * | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 2 | 0.05 | 1 | 0.02 | 3 | 0.07 | 3 | 0.07 | 1 | 0.02 | 2 | 0.05 | 2 | 0.03 |
| Cyprus | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.11 | 0 | 0 |
| Czechia | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 1 | 0.01 | 4 | 0.04 | 4 | 0.04 | 0 | 0 | 1 | 0.01 | 0 | 0 |
| Denmark | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * |
| Estonia | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.08 | 1 | 0.08 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0.02 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | 20 | 0 | 21 | 0 | 28 | 0 | 19 | 0 | 14 | 0 | 17 | 0.03 | 19 | 0.03 | 21 | 0.03 | 26 | 0.04 | 34 | 0.05 | 19 | 0.03 | 21 | 3 | 37 | 0.05 |
| Germany | 22 | 0 | 24 | 0 | 28 | 0 | 26 | 0 | 45 | 0.1 | 44 | 0.05 | 36 | 0.04 | 41 | 0.05 | 37 | 0.04 | 36 | 0.04 | 19 | 0.02 | 13 | 0.02 | 35 | 0.04 |
| Greece | 97 | 0.9 | 98 | 0.9 | 123 | 1.1 | 159 | 1.4 | 135 | 1.2 | 109 | 1 | 119 | 1.1 | 94 | 0.87 | 97 | 0.9 | 65 | 0.61 | 30 | 0.28 | 24 | 0.22 | 35 | 0.33 |
| Hungary | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Iceland | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ireland | 1 | 0 | 1 | 0 | 2 | 0 | 1 | 0 | 3 | 0.1 | 0 | 0 | 2 | 0.04 | 2 | 0.04 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.02 |
| Italy | 171 | 0.3 | 166 | 0.3 | 184 | 0.3 | 137 | 0.2 | 8 | * | 105 | 0.17 | 211 | 0.35 | 99 | 0.16 | 94 | 0.16 | 49 | 0.08 | 18 | 0.03 | 32 | 0.05 | 20 | 0.03 |
| Latvia | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.05 | 0 | 0 | 0 | 0 |
| Liechtenstein | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | * | 0 | 0 | 0 | 0 |
| Lithuania | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | 1 | 0.2 | 1 | 0.2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.16 | 1 | 0.15 |
| Malta | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | 6 | 0 | 1 | 0 | 3 | 0 | 5 | 0 | 1 | 0 | 7 | 0.04 | 5 | 0.03 | 2 | 0.01 | 5 | 0.03 | 7 | 0.04 | 2 | 0.01 | 2 | 0.01 | 5 | 0.03 |
| Norway | 2 | 0 | 2 | 0 | 4 | 0.1 | 2 | 0 | 2 | 0 | 2 | 0.04 | 4 | 0.08 | 3 | 0.06 | 3 | 0.06 | 4 | 0.08 | 2 | 0.04 | 3 | 0.06 | 1 | 0.02 |
| Poland | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 4 | 0.01 | 3 | 0.01 | 2 | 0.01 | 0 | 0 | 2 | 0.01 | 0 | 0 | 1 | 0 | 1 | 0 |
| Portugal | 88 | 0.8 | 76 | 0.7 | 37 | 0.4 | 22 | 0.2 | 50 | 0.5 | 46 | 0.44 | 50 | 0.48 | 16 | 0.16 | 19 | 0.18 | 33 | 0.32 | 9 | 0.09 | 10 | 0.1 | 13 | 0.13 |
| Romania | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 1 | 0.01 | 3 | 0.02 | 1 | 0.01 | 1 | 0.01 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovakia | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0.02 | 1 | 0.02 | 1 | 0.02 | 0 | 0 | 1 | 0.02 | 2 | 0.04 | 6 | 0.11 | 3 | 0.06 |
| Slovenia | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.05 | 1 | 0.05 | 3 | 0.15 | 6 | 0.29 | 1 | 0.05 | 0 | 0 | 1 | 0.05 |
| Spain | 78 | 0.2 | 43 | 0.1 | 62 | 0.1 | 87 | 0.2 | 60 | 0.1 | 33 | 0.07 | 37 | 0.08 | 63 | 0.13 | 40 | 0.09 | 20 | 0.04 | 10 | 0.07 | 25 | * | 22 | 0.05 |
| Sweden | 12 | 0.1 | 11 | 0.1 | 13 | 0.1 | 10 | 0.1 | 16 | 0.2 | 13 | 0.13 | 19 | 0.19 | 14 | 0.14 | 11 | 0.11 | 14 | 0.14 | 7 | 0.03 | 10 | 0.1 | 10 | 0.1 |
| United Kingdom | 12 | 0 | 25 | 0 | 14 | 0 | 15 | 0 | 11 | 0 | 12 | 0.02 | 14 | 0.02 | * | * | * | * | 24 | 0.04 | * | * | * | * | * | * |
| EU/EEA | 519 | 0.1 | 483 | 0.1 | 507 | 0.1 | 496 | 0.1 | 354 | 0.1 | 439 | 0.09 | 534 | 0.1 | 381 | 0.09 | 361 | 0.08 | 313 | 0.06 | 134 | 0.03 | 165 | 0.04 | 199 | 0.04 |
Abbreviations: RC: Reported cases; N: Number; R: Rate;
Source: ECDC - Annual epidemiological reports: Brucellosis3.
*Data presented include all officially registered human cases reported and noted in the annual epidemiological reports by ECDC.
Data presented in Table 2 showed that for the investigated period, the highest share of human cases was reported by 4 countries – Greece, Italy, Portugal, and Spain.
Sporadic cases have been identified in 10 countries - Croatia, the Czech Republic, Estonia, Finland, Iceland, Ireland, Latvia, Lithuania, Luxembourg, Malta. The disease has not been detected throughout the whole period in 3 countries – Denmark, Hungary, and Liechtenstein, and in Cyprus, there was only one case in a patient in 2021.
The number of reported brucellosis cases decreased to the lowest level in 2017, since the beginning of coordinated surveillance at the EU level in 2007, highlighting successful intervention measures [23].
The notification rate in Bulgaria also varied (from 0.05 in 2015 to 0.01 in 2018 and 0.03 in 2022), but it should be emphasized that its values are in a decreasing trend, and compared to the values for EU/EEA countries, this rate is average.
The vast epidemiological data provided over the past decade are helpful for the preparation of a new mapping of human brucellosis worldwide, taking into consideration multiple complex sanitary, socio-economic, and political conditions. The intensified international trade and travel, it significantly affect brucellosis management, as the disease is observed at high rates in many regions, including South America, Africa, the Middle East, and many parts of Asia [24].
4. LIMITATIONS
Several limitations should be considered when interpreting the presented findings. The study relied exclusively on officially reported and laboratory-confirmed cases and outbreaks. Underreporting of human brucellosis is well documented globally, particularly in regions where mild or non-specific clinical presentations may not necessitate laboratory testing. Therefore, the true incidence in Bulgaria may be underestimated.
Additionally, species-level differentiation of Brucella isolates in human cases was not consistently available in the national surveillance database. Although Brucella melitensis is considered the predominant species in the region, the absence of systematic species identification limits precise attribution of zoonotic transmission pathways. Furthermore, genomic sequencing data were not routinely available for paired human and animal isolates during most of the study period. Consequently, epidemiological links between animal outbreaks and subsequent human cases were inferred temporally and geographically rather than confirmed by molecular typing.
The concentration of surveillance efforts and diagnostic awareness in border districts following previous outbreaks may have introduced detection bias. Increased case-finding intensity in these regions could partially explain the higher observed incidence compared with interior districts.
Finally, the regression analysis was based on aggregated annual data and did not account for potential confounders such as district population size, livestock density, occupational structure, or cross-border mobility patterns. Therefore, the identified associations should be interpreted as indicative rather than causal.
CONCLUSION
The emergence and re-emergence of brucellosis in Bulgaria, the EU, and globally demonstrate gaps in the implementation of preventive and surveillance measures. Despite continuous achievements in laboratory research and diagnostics of sick and contact people and animals, brucellosis remains a serious threat to public health. Complete eradication will require more effective epidemiological investigations and, above all, their coordinated implementation by competent public health and veterinary authorities within a One Health framework. An important emphasis in improving surveillance measures is collecting data on sick people during the recovery period and on people living in rural areas.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.R., R.N., G.B., and I.T.: Study conception and design; R.R., R.N., G.B., and I.T.: Data collection; R.R., R.N., G.B., and I.T.: Analysis and interpretation of results; R.R., R.N., G.B., and I.T.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| NRL EDBI | = National Reference Laboratory “Especially Dangerous Bacterial Infections |
| NCPHA | = National Center for Public Health and Analyses |
| NCIPD | = National Center of Infectious and Parasitic Diseases |
| EFSA | = European Food Safety Authority |
| WAHIS | = World Animal Health Information System |
| ECDC | = European Centre for Disease Prevention and Control |
| LRV | = Large Ruminants |
| SRV | = Small Ruminants |
| RFSD | = Regional Food Safety Directorates |
| FBSA | = Bulgarian Food Safety Agency |
| ADIS | = Animal Disease Information System |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [R.R] upon reasonable request.
FUNDING
This research was funded by the Ministry of Education and Science in Bulgaria within the framework of the Bulgarian National Recovery and Resilience Plan, Component “Innovative Bulgaria”, Project No. BG-RRP-2.004-0006-C02 “Development of research and innovation at Trakia University in the service of health and sustainable well-being”. The authors extend their gratitude to the Faculty of Veterinary Medicine and Trakia University, Stara Zagora, Bulgaria for the financial support provided for this paper’s publication.
ACKNOWLEDGEMENTS
Declared none.

